

Minimally invasive resection of an extradural far lateral lumbar schwannoma with zygapophyseal joint sparing: surgical nuances and literature review
- PMID: 25328530
- PMCID: PMC4189855
- DOI: 10.1155/2014/739862
Minimally invasive resection of an extradural far lateral lumbar schwannoma with zygapophyseal joint sparing: surgical nuances and literature review
Abstract
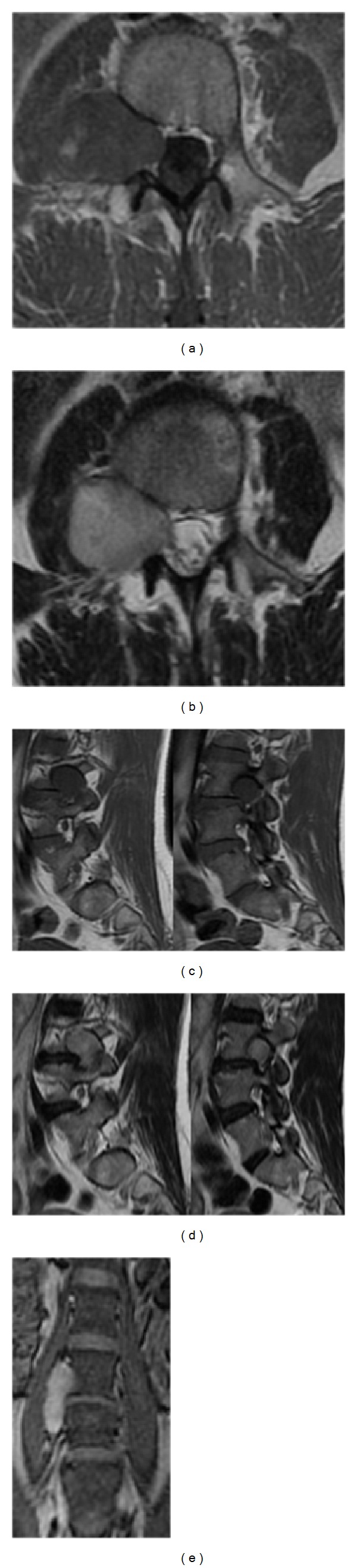
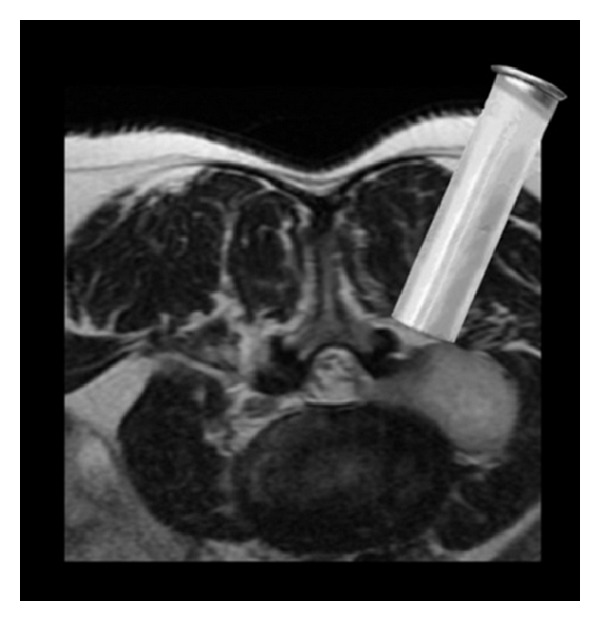
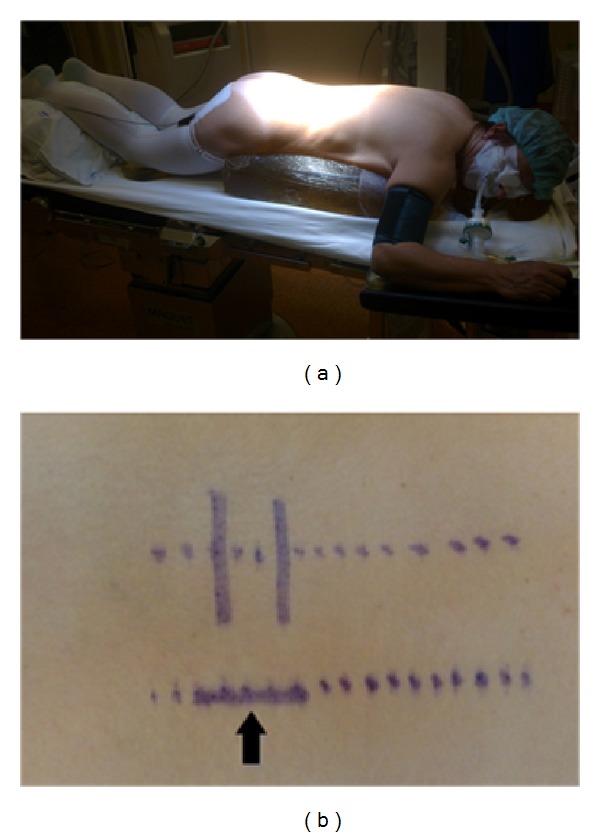
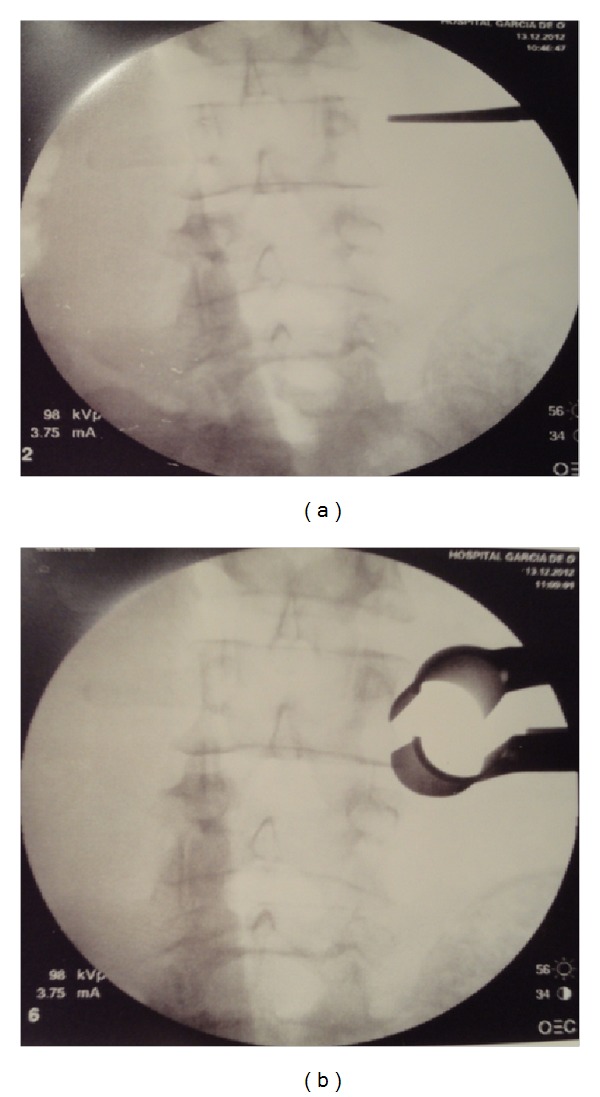
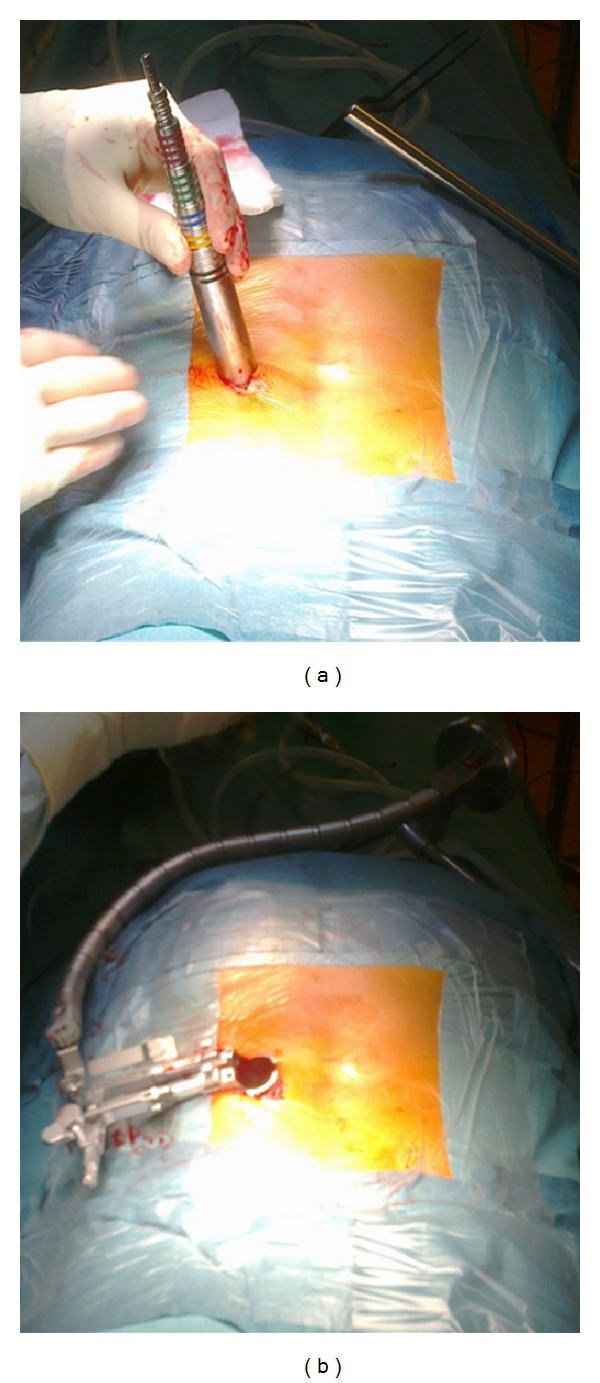
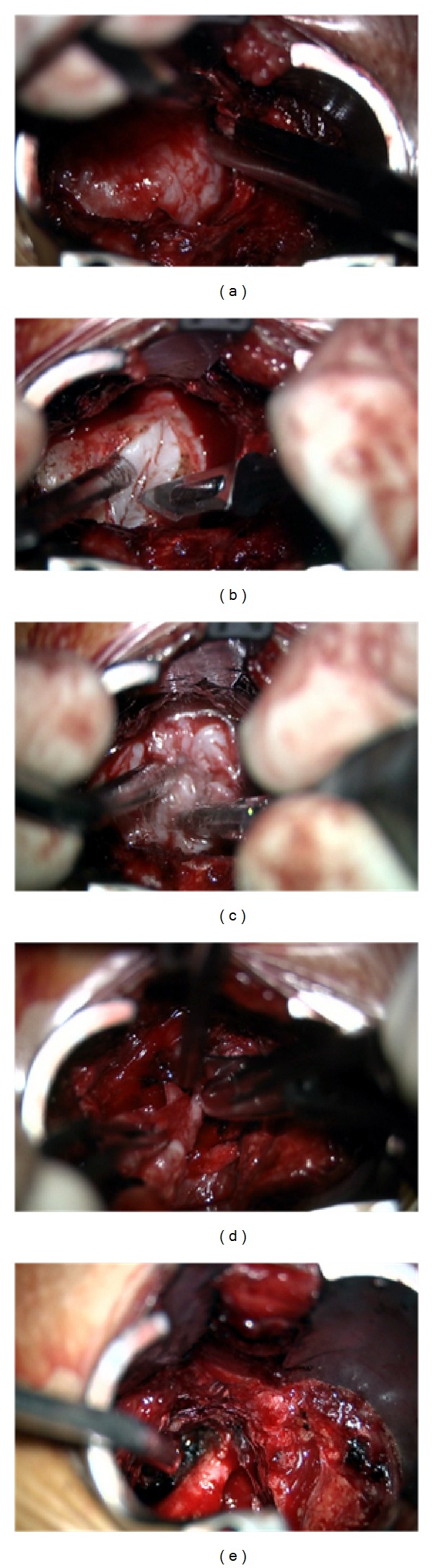
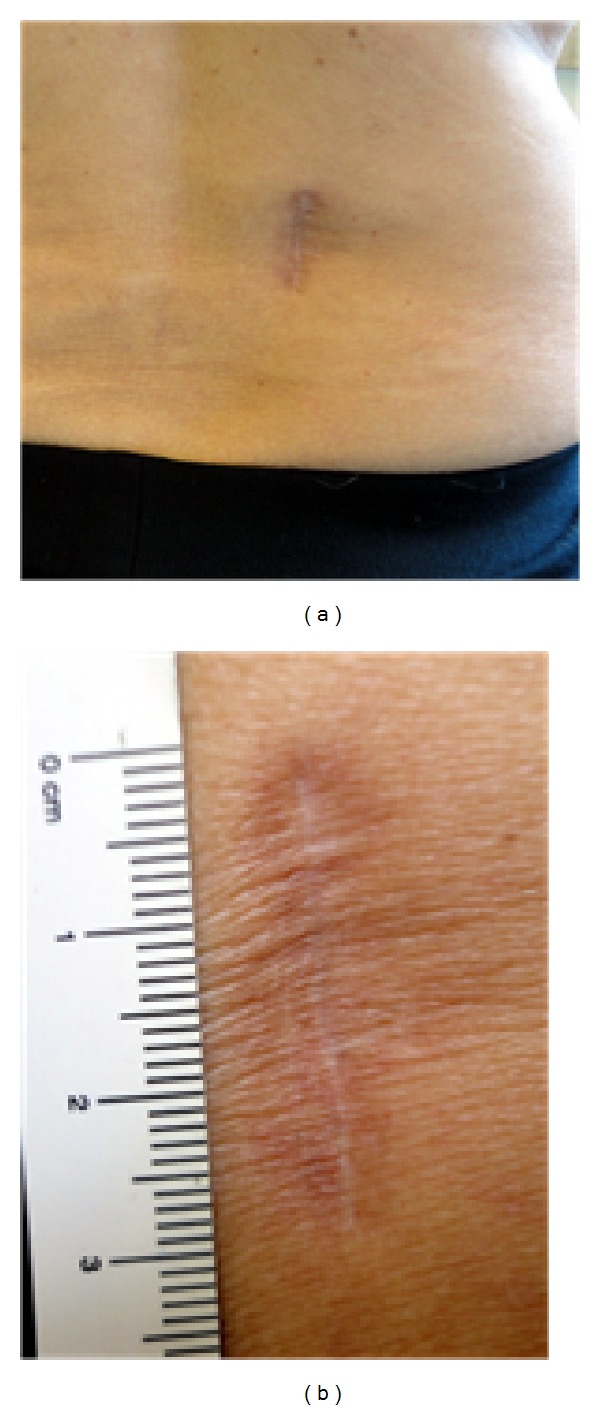
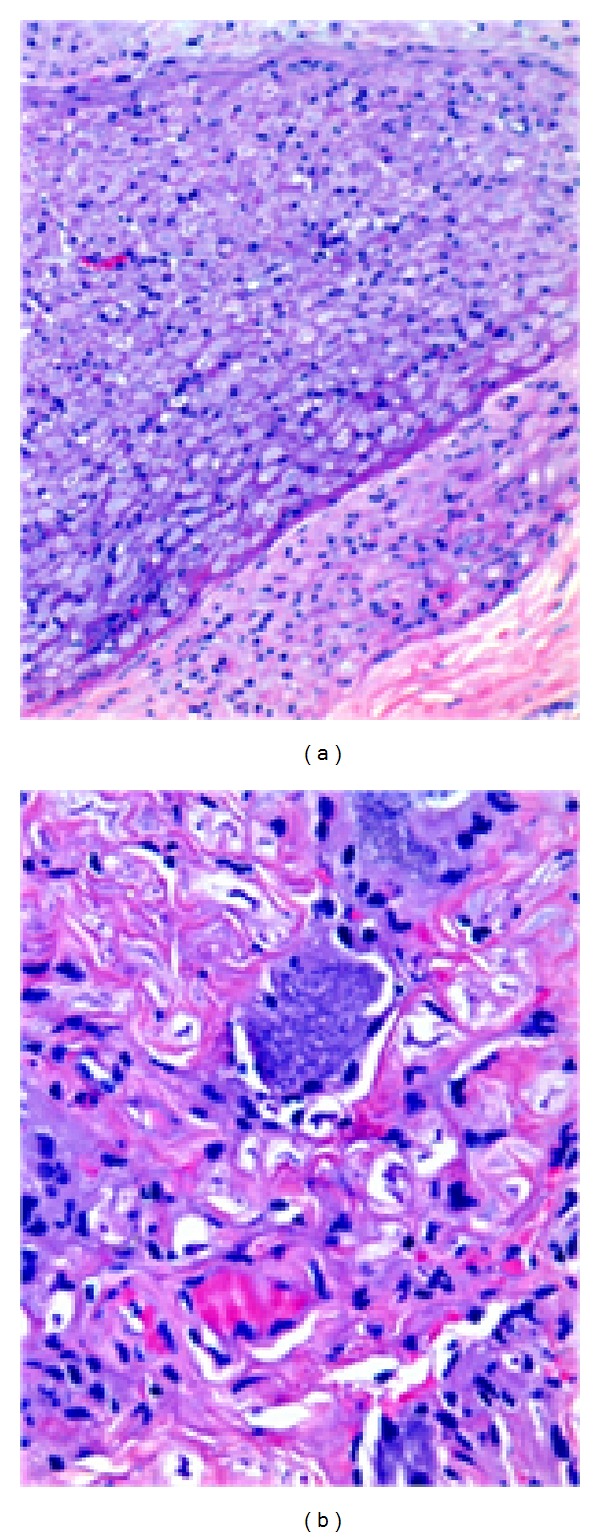
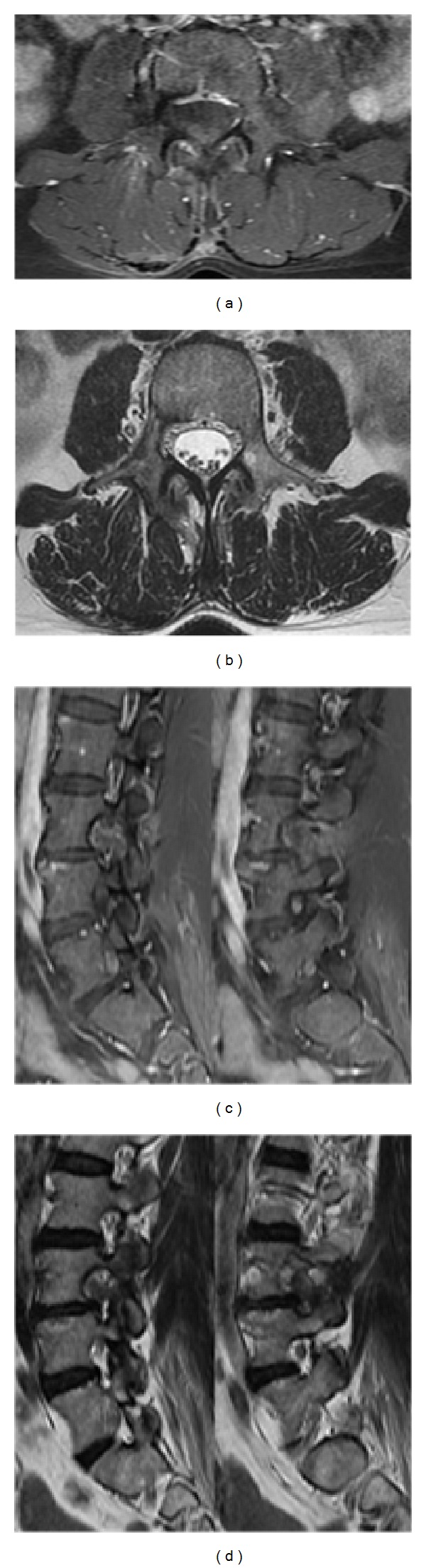
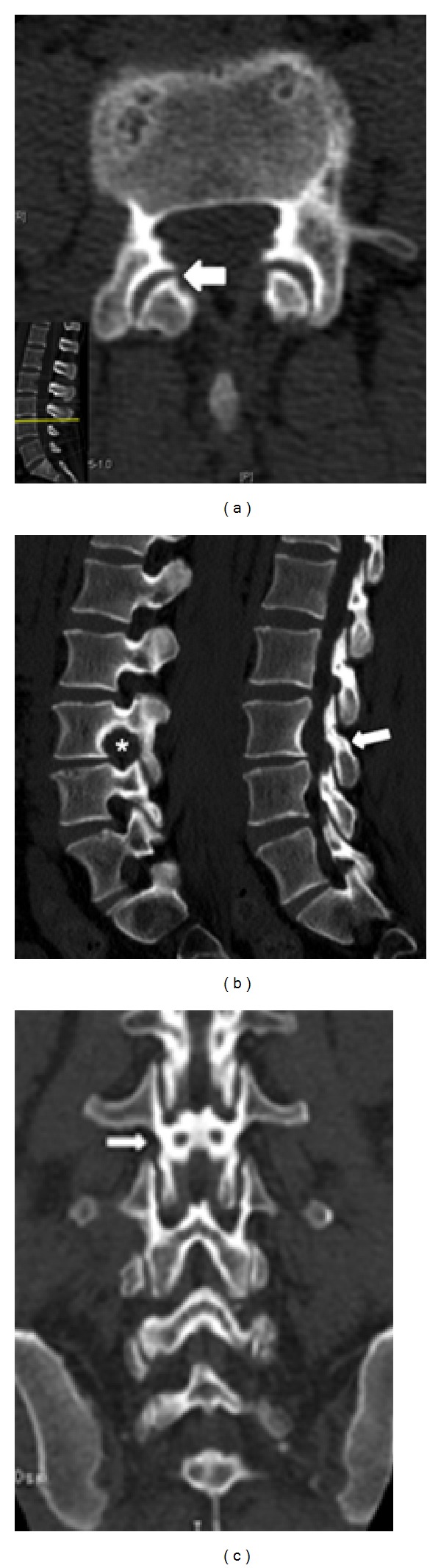
Introduction. Spinal schwannomas are benign nerve sheath tumors. Completely extradural schwannomas of the lumbar spine are extremely rare lesions, accounting for only 0,7-4,2% of all spinal NSTs. Standard open approaches have been used to treat these tumors, requiring extensive muscle dissection, laminectomy, radical foraminotomy, and facetectomy. In this paper the authors present the case of a minimally invasive resection of a completely extradural schwannoma. Operative technique literature review is presented. Material & Methods. A 50-year-old woman presented with progressive complains of chronic right leg pain and paresthesia. The magnetic resonance imaging revealed a giant well-encapsulated dumbbell-shaped extradural lesion at the L3-L4 level. The patient underwent a minimally invasive gross total resection of the tumor using a tubular expandable retractor system. Results. The patient had complete resolution of radiculopathy in the immediate postoperative period and she was discharged home, neurologically intact, on the second postoperative day. Postoperative MRI demonstrated no evidence of residual tumor. At latest follow-up (18 months) the patient remains asymptomatic. Conclusion. Although challenging, this minimally invasive procedure is safe and effective, being an appropriate alternative, with many potential advantages, to the open approach.
Figures
References
-
- Nittner K, Vinken PH, Bruyn GW, editors. Handbook of Clinical Neurology. New York, NY, USA: North Holland, Amsterdam, The Netherlands; Elsevier; 1976. Spinal meningiomas , neuromas and neurofibromas, and hourglass tumors; pp. 177–322.
-
- Jinnai T, Hoshimaru M, Koyama T. Clinical characteristics of spinal nerve sheath tumors: analysis of 149 cases. Neurosurgery. 2005;56(3):510–515. - PubMed
-
- Greenberg MS. Handbook of Neurosurgery. Thieme; 2010. Spinal schwannomas; pp. 734–736.
-
- Celli P, Trillò G, Ferrante L. Spinal extradural schwannoma. Journal of Neurosurgery Spine. 2005;2(4):447–456. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
