

Chronic neck pain: making the connection between capsular ligament laxity and cervical instability
- PMID: 25328557
- PMCID: PMC4200875
- DOI: 10.2174/1874325001408010326
Chronic neck pain: making the connection between capsular ligament laxity and cervical instability
Abstract
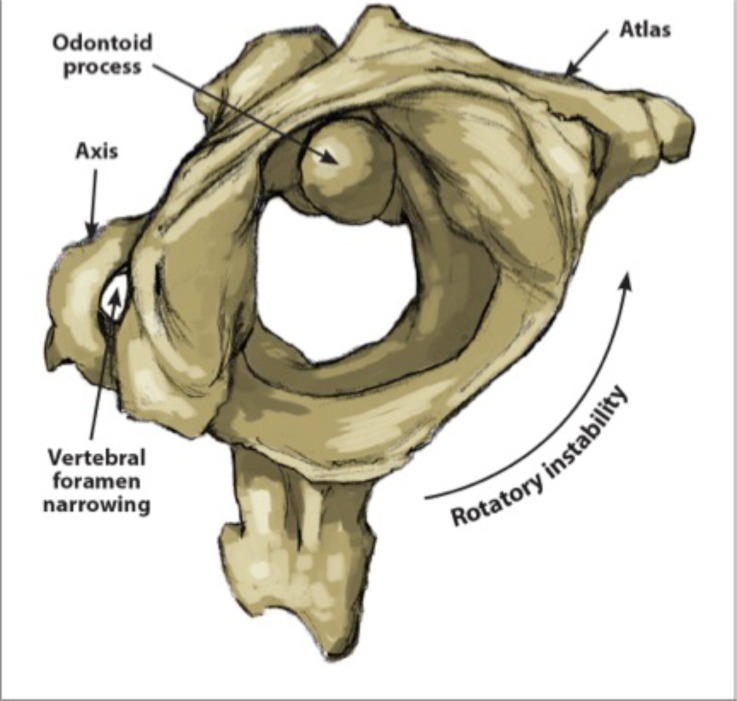
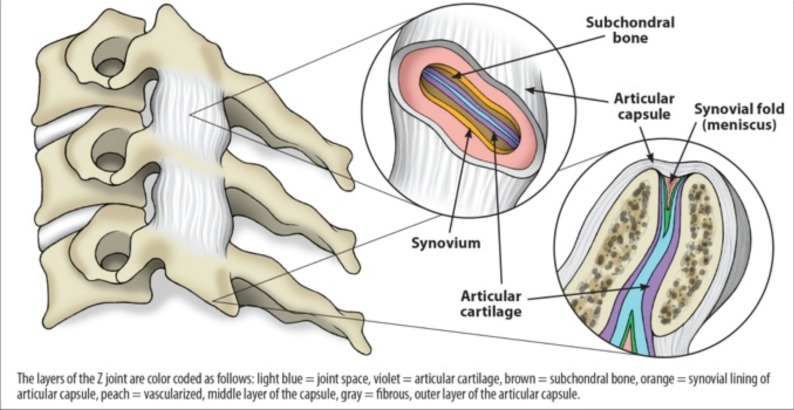
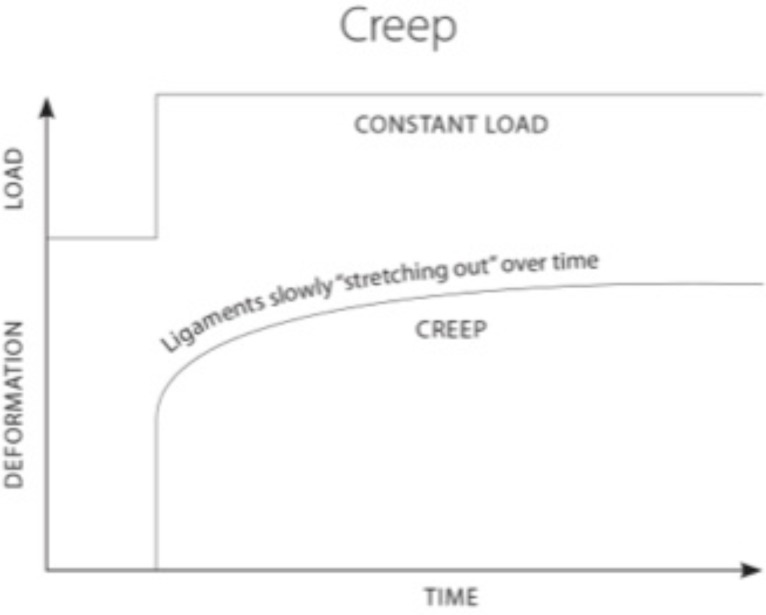
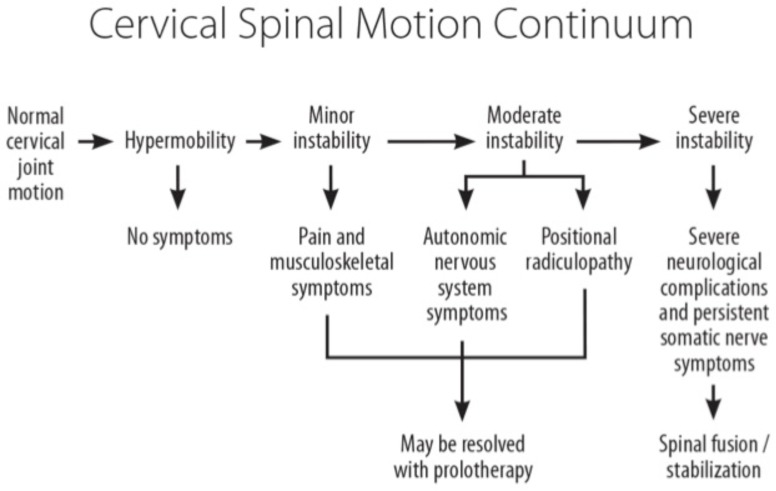
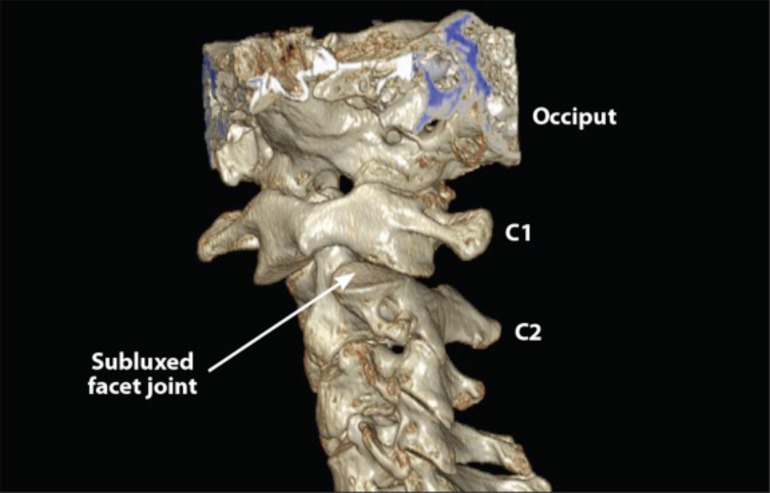
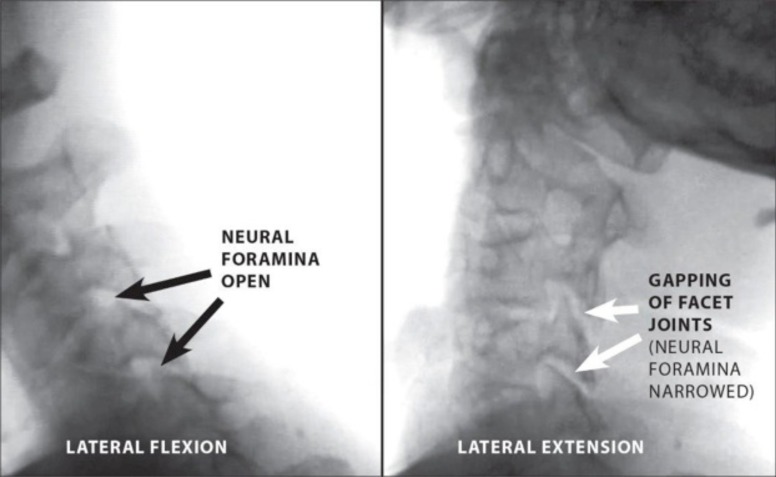
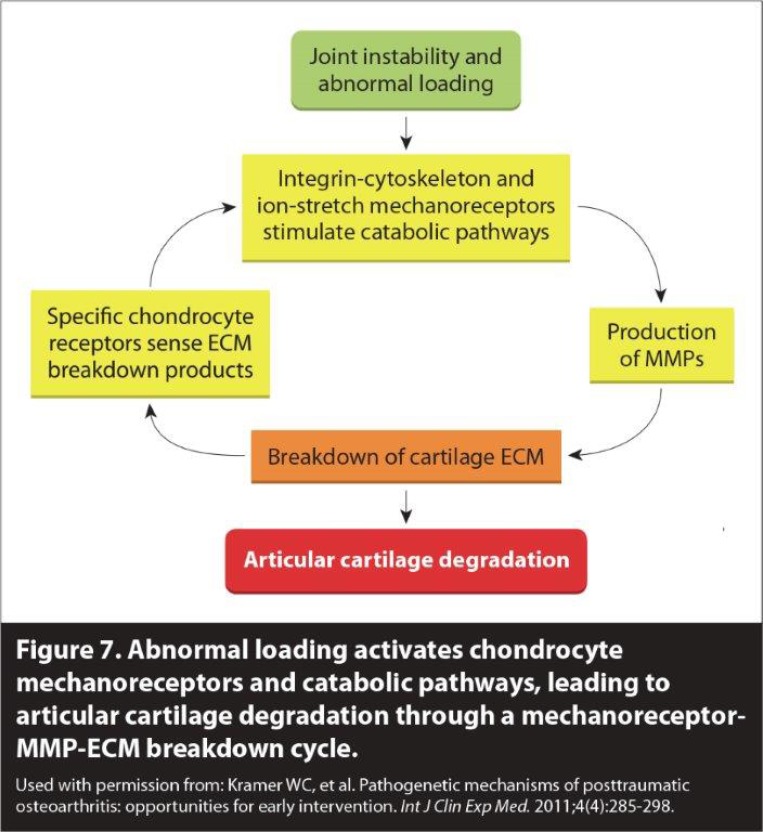
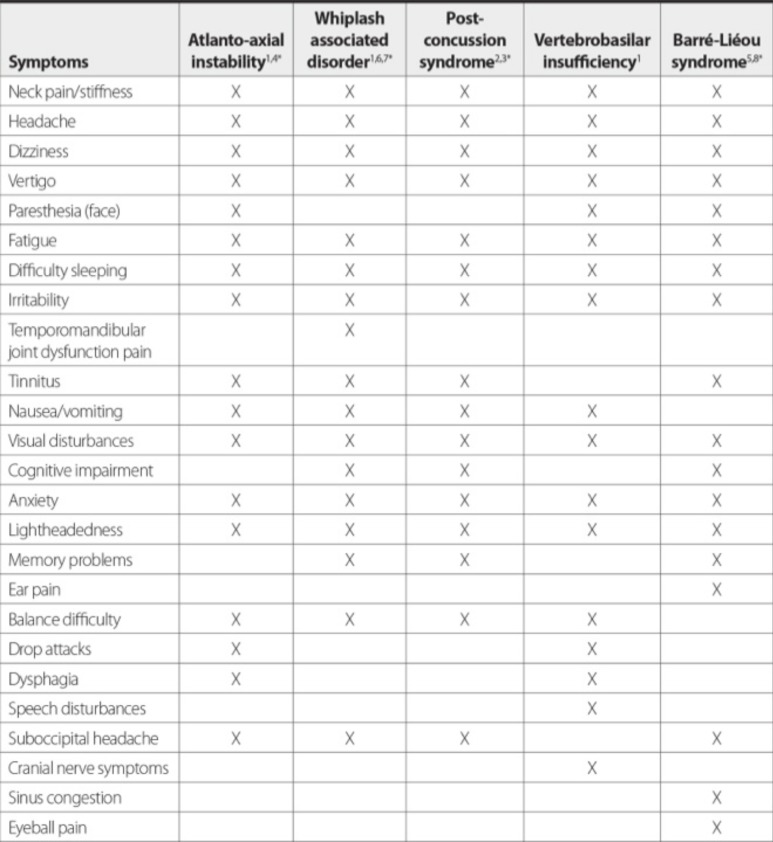
The use of conventional modalities for chronic neck pain remains debatable, primarily because most treatments have had limited success. We conducted a review of the literature published up to December 2013 on the diagnostic and treatment modalities of disorders related to chronic neck pain and concluded that, despite providing temporary relief of symptoms, these treatments do not address the specific problems of healing and are not likely to offer long-term cures. The objectives of this narrative review are to provide an overview of chronic neck pain as it relates to cervical instability, to describe the anatomical features of the cervical spine and the impact of capsular ligament laxity, to discuss the disorders causing chronic neck pain and their current treatments, and lastly, to present prolotherapy as a viable treatment option that heals injured ligaments, restores stability to the spine, and resolves chronic neck pain. The capsular ligaments are the main stabilizing structures of the facet joints in the cervical spine and have been implicated as a major source of chronic neck pain. Chronic neck pain often reflects a state of instability in the cervical spine and is a symptom common to a number of conditions described herein, including disc herniation, cervical spondylosis, whiplash injury and whiplash associated disorder, postconcussion syndrome, vertebrobasilar insufficiency, and Barré-Liéou syndrome. When the capsular ligaments are injured, they become elongated and exhibit laxity, which causes excessive movement of the cervical vertebrae. In the upper cervical spine (C0-C2), this can cause a number of other symptoms including, but not limited to, nerve irritation and vertebrobasilar insufficiency with associated vertigo, tinnitus, dizziness, facial pain, arm pain, and migraine headaches. In the lower cervical spine (C3-C7), this can cause muscle spasms, crepitation, and/or paresthesia in addition to chronic neck pain. In either case, the presence of excessive motion between two adjacent cervical vertebrae and these associated symptoms is described as cervical instability. Therefore, we propose that in many cases of chronic neck pain, the cause may be underlying joint instability due to capsular ligament laxity. Currently, curative treatment options for this type of cervical instability are inconclusive and inadequate. Based on clinical studies and experience with patients who have visited our chronic pain clinic with complaints of chronic neck pain, we contend that prolotherapy offers a potentially curative treatment option for chronic neck pain related to capsular ligament laxity and underlying cervical instability.
Keywords: Atlanto-axial joint; Barré- Liéou syndrome; C1-C2 facet joint; capsular ligament laxity; cervical instability; cervical radiculopathy; chronic neck pain; facet joints; post-concussion syndrome; prolotherapy; spondylosis; vertebrobasilar insufficiency; whiplash..
Figures
References
-
- Childs J, Cleland J, Elliott J , et al. Neck pain clinical practice guidelines linked to the international classification of functioning, disability, and health from the orthopaedic section of the American Physical Therapy Association. J Orthop Sports Phys Ther. 2008;38(9): A1–34. - PubMed
-
- Côté P, Cassidy JD, Carroll LJ, Kristman V. The annual incidence and course of neck pain in the general population a population based cohort study. Pain. 2004;112(3): 267–73. - PubMed
-
- Hogg-Johnson S, van der Velde G, Carroll LJ , et al. The burden and determinants of neck pain in the general population. Eur Spine J. 2008;17(Suppl 1 ): 39–51. - PubMed
-
- Childs JD, Fritz JM, Flynn TW , et al. A clinical prediction rule to identify patients with low back pain most likely to benefit from spinal manipulation a validation study. Ann Intern Med. 2004;141(12): 920–8. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous