

Treatment of nonspecific thoracic spine pain with trigger point dry needling and intramuscular electrical stimulation: a case series
- PMID: 25328832
- PMCID: PMC4196334
Treatment of nonspecific thoracic spine pain with trigger point dry needling and intramuscular electrical stimulation: a case series
Abstract
Study design: Case Series.
Background and purpose: Myofascial trigger points (MTrPs) are a common occurrence in many musculoskeletal issues and have been shown to be prevalent in both subjects with nonspecific low back pain and whiplash associated disorder. Trigger point dry needling (DN) has been shown to reduce pain and improve function in areas such as the cervical and lumbar spine, shoulder, hip, and knee, but has not been investigated in the thoracic spine. The purpose of this case series was to document the use of DN with intramuscular electrical stimulation (IES) in subjects with nonspecific thoracic spine pain.
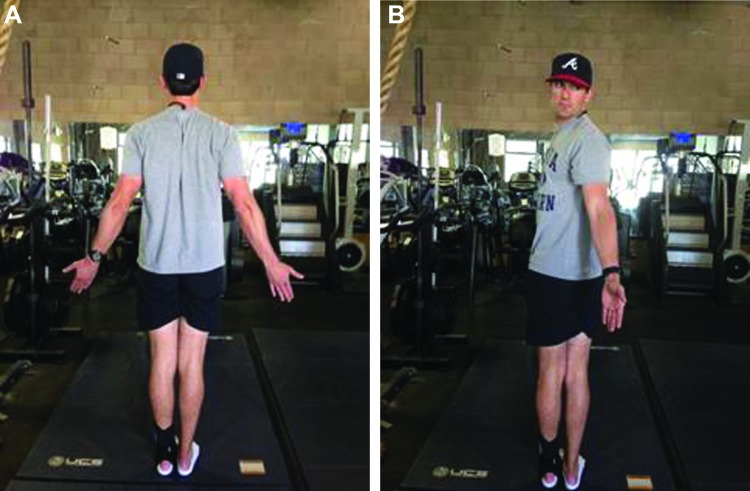
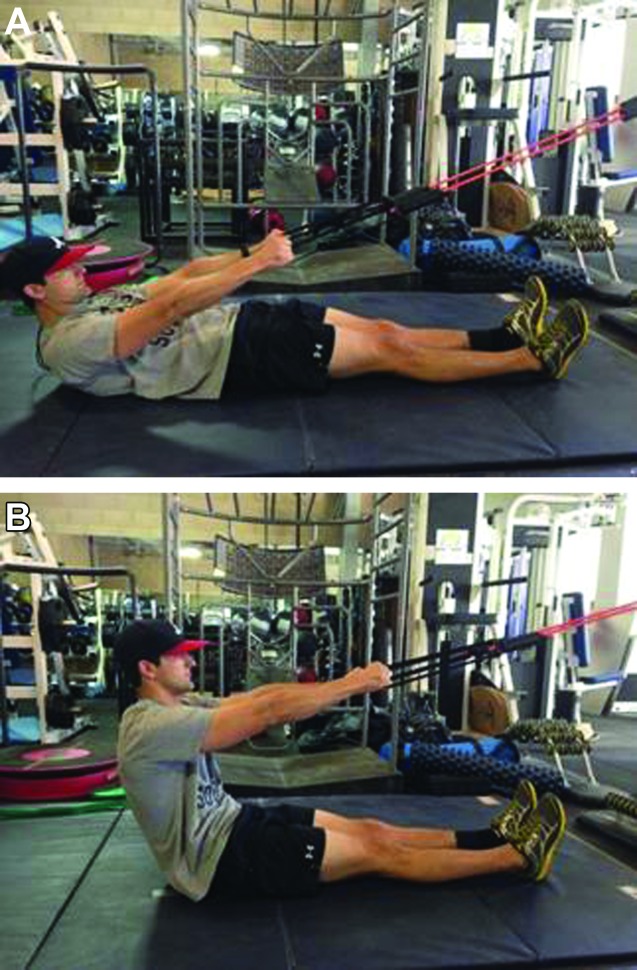
Case description: The subjects were both active duty military males aged 31 and 27 years who self-referred to physical therapy for thoracic spinal pain. Physical examination demonstrated thoracic motor control dysfunction, tissue hypertonicity, and tenderness to palpation of bilateral thoracic paraspinal musculature in both subjects. This indicated the presence of possible MrTPs. Objective findings in the first subject included painful thoracic flexion and bilateral rotation in each of these planes of movement. Pain reduction was observed when postural demands of the spine and trunk musculature were reduced through positional changes. Patient 1 demonstrated pain with posterior to anterior (P/A) pressure at T9 to T12. The second subject had bilaterally limited and painful thoracic rotation actively with normal passive rotation and demonstrated pain with P/A pressure at T4 to T7.
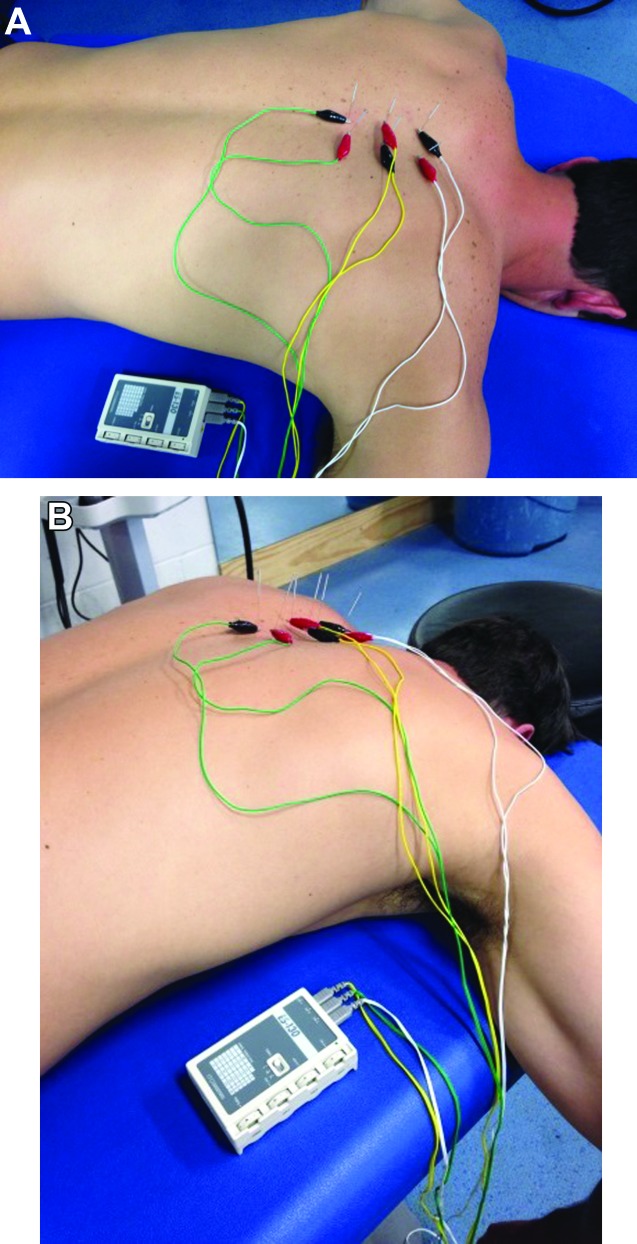
Intervention: The subjects were treated with DN and IES for a total of two visits each. DN was performed to paraspinal and multifidus musculature at the levels of elicited pain with P/A testing and IES set at a frequency level of 4 (1.5Hz) for 20 minutes.
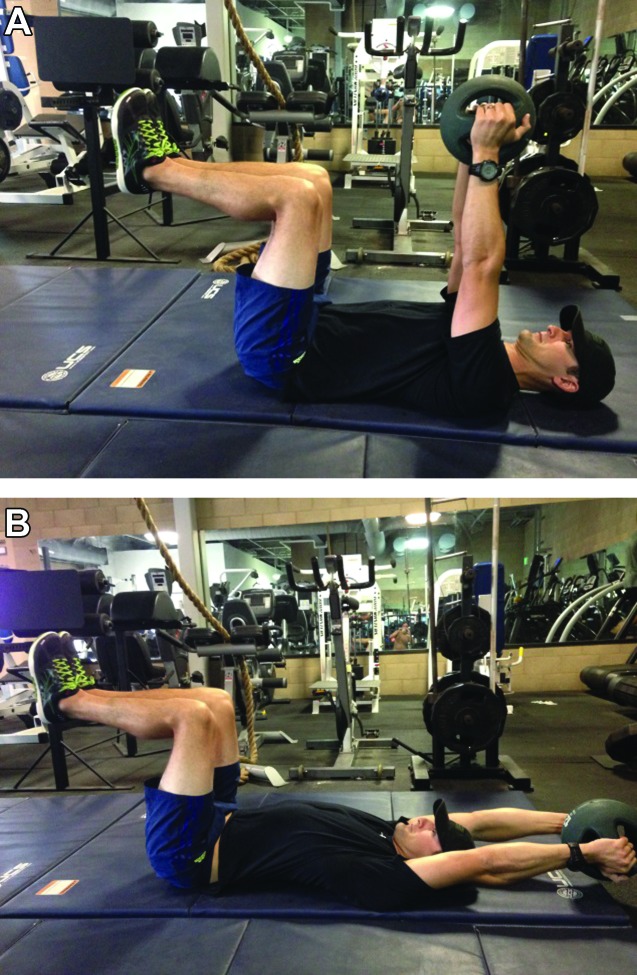
Outcomes: Subject 1 reported reduced pain with standing flexion from a 62mm VAS score on initial evaluation to 26mm at his second visit. Subject 2 reported being "quite a bit better" in symptoms on the GROC following his second treatment. His VAS score reported following weightlifting activities changed from 43mm on initial evaluation to 20mm at his second visit. Both subjects also demonstrated a 10 degree improvement in active thoracic spinal rotation (on the right for Subject 1 and bilateral for Subject 2) following their second treatment.
Discussion: Both subjects demonstrated motor control dysfunctions and pain with P/A pressure in the thoracic spine. With the use of DN and IES, immediate reduction was seen in subject perceived symptoms, and pain free ROM was improved. Extended treatment and follow up was not plausible due to the high pace tempo and demands of their operational training schedule. With research indicating the influence of MTrPs on a multitude of musculoskeletal issues and the prevalence of thoracic spine pain, further research is indicated for examining the effects of DN and IES for motor control and painful conditions occurring in the thoracic spine.
Level of evidence: Level 4.
Keywords: Dry needling; intramuscular electrical stimulation; myofasical trigger points; thoracic spine pain.
Figures





References
-
- Briggs AM Bragge P Smith AJ Gouil D Straker LM Prevelence and associated factors for thoracic spine pain in the adult working population: a literature review. J Occup Health. 2009;51: 177‐192 - PubMed
-
- Wood KB Garvey TA Gundry C Heithoff KB Magnetic resonance imaging of the thoracic spine. Evaluation of asymptomatic individuals. J Bone Joint Surg Am. 1995;77(11):1631‐1638 - PubMed
LinkOut - more resources
Full Text Sources
Medical
Research Materials