

Does this chest radiograph belong to a survivor of childhood cancer? Radiographic findings suggesting previous treatment for childhood cancer - a review
Affiliations
- PMID: 25328855
- PMCID: PMC4201239
Item in Clipboard
Does this chest radiograph belong to a survivor of childhood cancer? Radiographic findings suggesting previous treatment for childhood cancer - a review
J Am Osteopath Coll Radiol.
2014 Apr.
Abstract
The growing population of long-term survivors of childhood cancer in the United States estimated in 2009 to be nearly 330,000 mandates familiarity with imaging findings that may be related to prior disease, therapy and toxicities. More than 24% of these patients have survived more than 30 years from the time of diagnosis of their malignancy. Thus, imagers of adult as well as pediatric patients should be cognizant of findings seen in this patient cohort. This image-based review will discuss findings demonstrated on chest radiographs that may suggest that the imaged patient is a childhood cancer survivor.
Figures

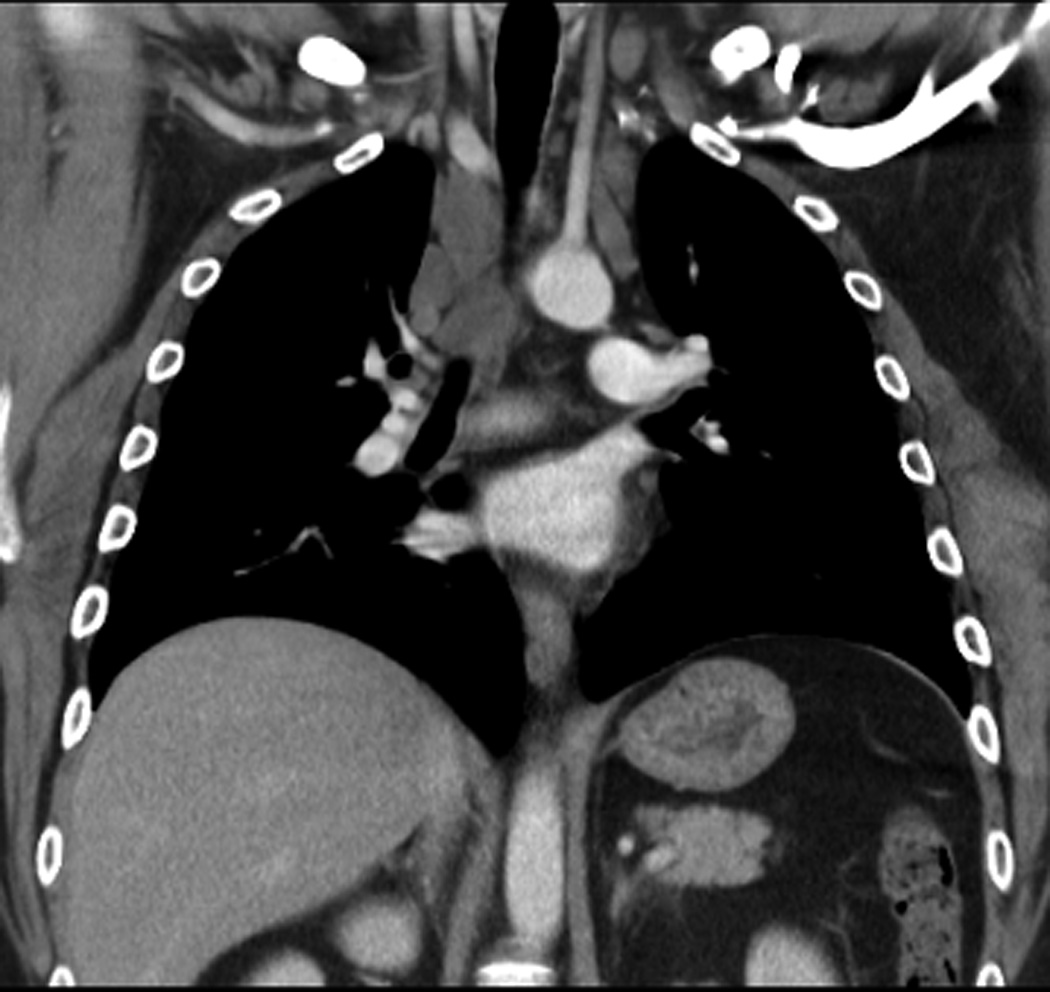
18-year-old man diagnosed with Stage IV B nodular sclerosing Hodgkin’s disease was treated with chemotherapy and 2550cGy mantle and 800 cGy whole lung irradiation. Residual mediastinal mass persisted over the subsequent 8 years from initial imaging at diagnosis through follow-up. A. Posteroanterior chest radiograph at the time of diagnosis shows a large anterior mediastinal mass which extends bilaterally from the midline. B and C. A follow-up posteroanterior chest radiograph obtained 8 years from diagnosis shows residual superior mediastinal widening that corresponds to the residual masses shown on the corresponding computed tomography image, C.

18-year-old man diagnosed with Stage IV B nodular sclerosing Hodgkin’s disease was treated with chemotherapy and 2550cGy mantle and 800 cGy whole lung irradiation. Residual mediastinal mass persisted over the subsequent 8 years from initial imaging at diagnosis through follow-up. A. Posteroanterior chest radiograph at the time of diagnosis shows a large anterior mediastinal mass which extends bilaterally from the midline. B and C. A follow-up posteroanterior chest radiograph obtained 8 years from diagnosis shows residual superior mediastinal widening that corresponds to the residual masses shown on the corresponding computed tomography image, C.
18-year-old man diagnosed with Stage IV B nodular sclerosing Hodgkin’s disease was treated with chemotherapy and 2550cGy mantle and 800 cGy whole lung irradiation. Residual mediastinal mass persisted over the subsequent 8 years from initial imaging at diagnosis through follow-up. A. Posteroanterior chest radiograph at the time of diagnosis shows a large anterior mediastinal mass which extends bilaterally from the midline. B and C. A follow-up posteroanterior chest radiograph obtained 8 years from diagnosis shows residual superior mediastinal widening that corresponds to the residual masses shown on the corresponding computed tomography image, C.

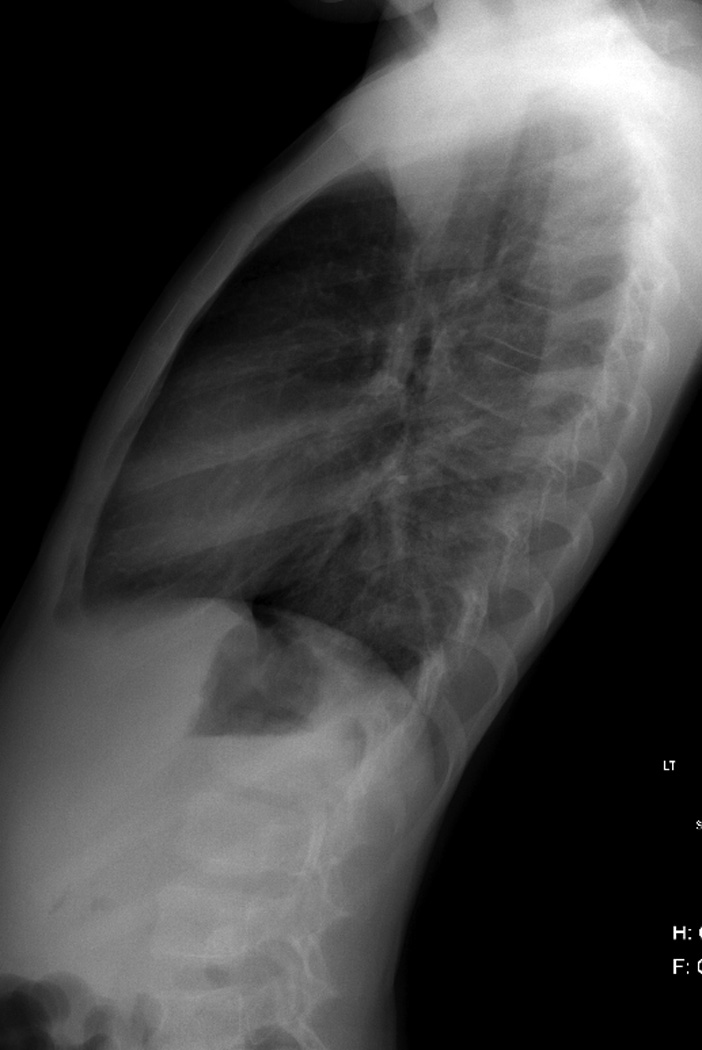
24-year-old survivor of Stage IIIB nodular sclerosing Hodgkin’s disease diagnosed at the age of 15-years. His disease was refractory to standard chemotherapy prompting autologous bone marrow transplantation and 2100 cGy mediastinal radiation. A and B. A, posteroanterior and, B, lateral chest radiographs at diagnosis show a bulky anterior mediastinal mass extending through the thoracic inlet on the right, into the right neck. C. C, Follow-up posteroanterior chest radiograph 6 years later show significant reduction in the mediastinal mass with development of dense calcifications.

24-year-old survivor of Stage IIIB nodular sclerosing Hodgkin’s disease diagnosed at the age of 15-years. His disease was refractory to standard chemotherapy prompting autologous bone marrow transplantation and 2100 cGy mediastinal radiation. A and B. A, posteroanterior and, B, lateral chest radiographs at diagnosis show a bulky anterior mediastinal mass extending through the thoracic inlet on the right, into the right neck. C. C, Follow-up posteroanterior chest radiograph 6 years later show significant reduction in the mediastinal mass with development of dense calcifications.

24-year-old survivor of Stage IIIB nodular sclerosing Hodgkin’s disease diagnosed at the age of 15-years. His disease was refractory to standard chemotherapy prompting autologous bone marrow transplantation and 2100 cGy mediastinal radiation. A and B. A, posteroanterior and, B, lateral chest radiographs at diagnosis show a bulky anterior mediastinal mass extending through the thoracic inlet on the right, into the right neck. C. C, Follow-up posteroanterior chest radiograph 6 years later show significant reduction in the mediastinal mass with development of dense calcifications.

24-year-old survivor of Stage IIIB nodular sclerosing Hodgkin’s disease diagnosed at the age of 15-years. His disease was refractory to standard chemotherapy prompting autologous bone marrow transplantation and 2100 cGy mediastinal radiation. A and B. A, posteroanterior and, B, lateral chest radiographs at diagnosis show a bulky anterior mediastinal mass extending through the thoracic inlet on the right, into the right neck. C. C, Follow-up posteroanterior chest radiograph 6 years later show significant reduction in the mediastinal mass with development of dense calcifications.
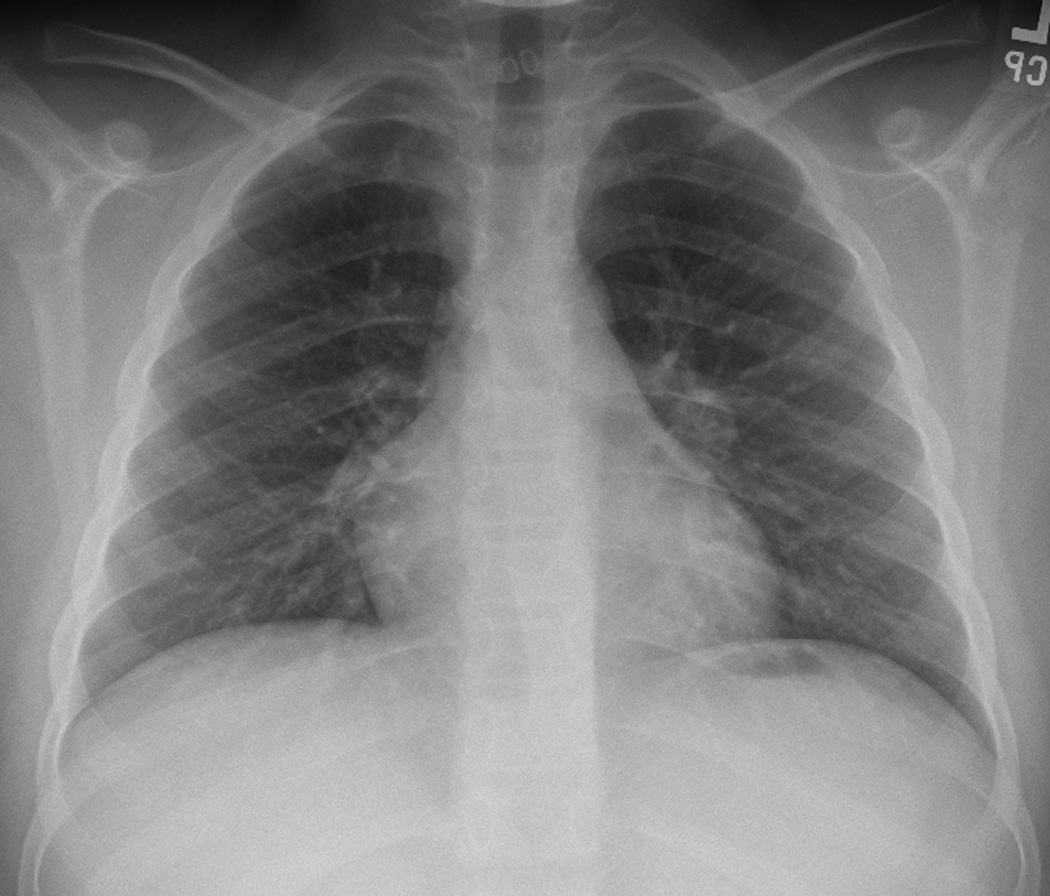
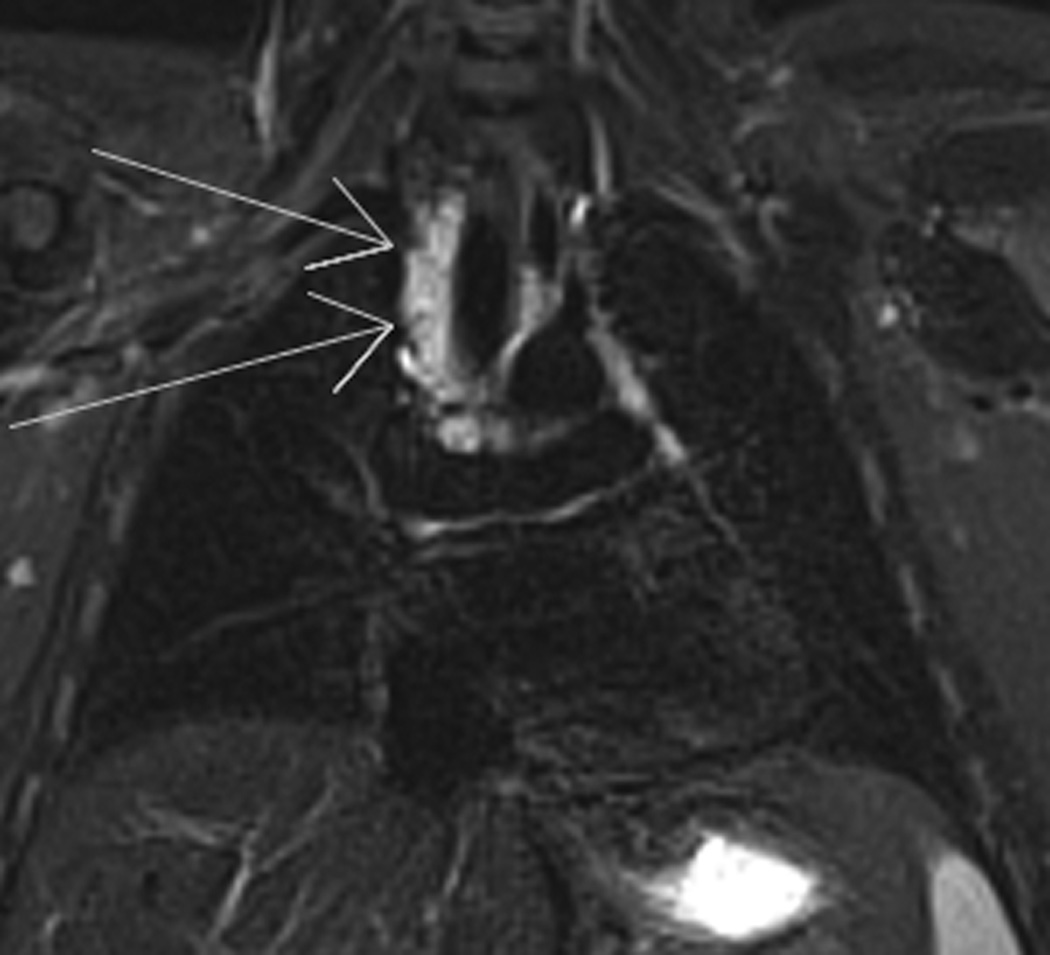
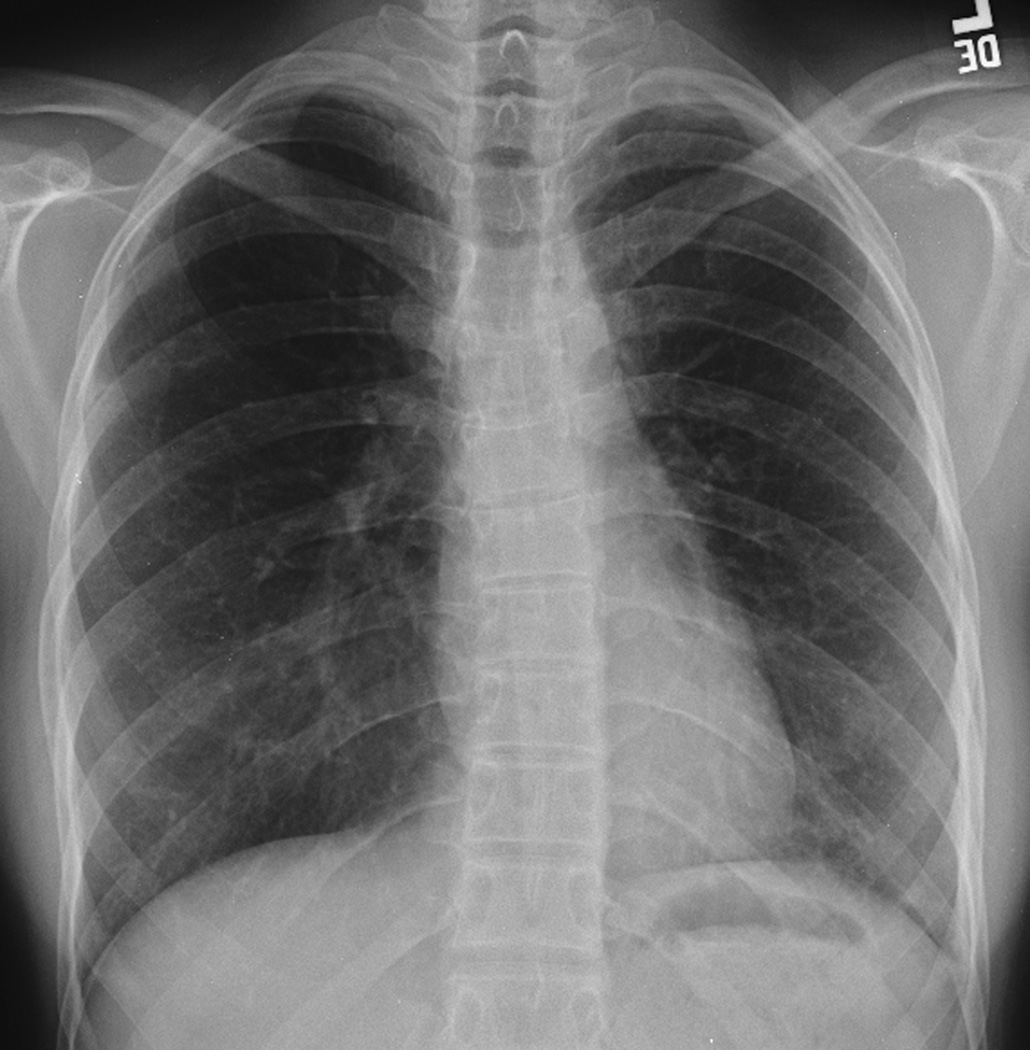
9-year-old boy diagnosed with Stage IA Hodgkin’s disease right neck achieved complete remission with chemotherapy. At routine follow-up 3.5 years later, left hilar relapse was suspected. A. and B. A, posteroanterior and lateral, B, chest radiographs show stable post-therapy appearance of the thoracic structures. C. and D. Posteroanterior chest radiograph shows slight increased density left hilum which, on the lateral view, D, is shown to represent an ovoid nodule (lines). E., and F., E, axial non-contrast T1- and, F, T2-weighted images of the chest show right paratracheal (long arrows), left hilar and subcarinal (short arrows) adenopathy consistent with disease relapse.

9-year-old boy diagnosed with Stage IA Hodgkin’s disease right neck achieved complete remission with chemotherapy. At routine follow-up 3.5 years later, left hilar relapse was suspected. A. and B. A, posteroanterior and lateral, B, chest radiographs show stable post-therapy appearance of the thoracic structures. C. and D. Posteroanterior chest radiograph shows slight increased density left hilum which, on the lateral view, D, is shown to represent an ovoid nodule (lines). E., and F., E, axial non-contrast T1- and, F, T2-weighted images of the chest show right paratracheal (long arrows), left hilar and subcarinal (short arrows) adenopathy consistent with disease relapse.

9-year-old boy diagnosed with Stage IA Hodgkin’s disease right neck achieved complete remission with chemotherapy. At routine follow-up 3.5 years later, left hilar relapse was suspected. A. and B. A, posteroanterior and lateral, B, chest radiographs show stable post-therapy appearance of the thoracic structures. C. and D. Posteroanterior chest radiograph shows slight increased density left hilum which, on the lateral view, D, is shown to represent an ovoid nodule (lines). E., and F., E, axial non-contrast T1- and, F, T2-weighted images of the chest show right paratracheal (long arrows), left hilar and subcarinal (short arrows) adenopathy consistent with disease relapse.

9-year-old boy diagnosed with Stage IA Hodgkin’s disease right neck achieved complete remission with chemotherapy. At routine follow-up 3.5 years later, left hilar relapse was suspected. A. and B. A, posteroanterior and lateral, B, chest radiographs show stable post-therapy appearance of the thoracic structures. C. and D. Posteroanterior chest radiograph shows slight increased density left hilum which, on the lateral view, D, is shown to represent an ovoid nodule (lines). E., and F., E, axial non-contrast T1- and, F, T2-weighted images of the chest show right paratracheal (long arrows), left hilar and subcarinal (short arrows) adenopathy consistent with disease relapse.

9-year-old boy diagnosed with Stage IA Hodgkin’s disease right neck achieved complete remission with chemotherapy. At routine follow-up 3.5 years later, left hilar relapse was suspected. A. and B. A, posteroanterior and lateral, B, chest radiographs show stable post-therapy appearance of the thoracic structures. C. and D. Posteroanterior chest radiograph shows slight increased density left hilum which, on the lateral view, D, is shown to represent an ovoid nodule (lines). E., and F., E, axial non-contrast T1- and, F, T2-weighted images of the chest show right paratracheal (long arrows), left hilar and subcarinal (short arrows) adenopathy consistent with disease relapse.

9-year-old boy diagnosed with Stage IA Hodgkin’s disease right neck achieved complete remission with chemotherapy. At routine follow-up 3.5 years later, left hilar relapse was suspected. A. and B. A, posteroanterior and lateral, B, chest radiographs show stable post-therapy appearance of the thoracic structures. C. and D. Posteroanterior chest radiograph shows slight increased density left hilum which, on the lateral view, D, is shown to represent an ovoid nodule (lines). E., and F., E, axial non-contrast T1- and, F, T2-weighted images of the chest show right paratracheal (long arrows), left hilar and subcarinal (short arrows) adenopathy consistent with disease relapse.

9-year-old boy diagnosed with Stage IA Hodgkin’s disease right neck achieved complete remission with chemotherapy. At routine follow-up 3.5 years later, left hilar relapse was suspected. A. and B. A, posteroanterior and lateral, B, chest radiographs show stable post-therapy appearance of the thoracic structures. C. and D. Posteroanterior chest radiograph shows slight increased density left hilum which, on the lateral view, D, is shown to represent an ovoid nodule (lines). E., and F., E, axial non-contrast T1- and, F, T2-weighted images of the chest show right paratracheal (long arrows), left hilar and subcarinal (short arrows) adenopathy consistent with disease relapse.
9-year-old boy diagnosed with Stage IA Hodgkin’s disease right neck achieved complete remission with chemotherapy. At routine follow-up 3.5 years later, left hilar relapse was suspected. A. and B. A, posteroanterior and lateral, B, chest radiographs show stable post-therapy appearance of the thoracic structures. C. and D. Posteroanterior chest radiograph shows slight increased density left hilum which, on the lateral view, D, is shown to represent an ovoid nodule (lines). E., and F., E, axial non-contrast T1- and, F, T2-weighted images of the chest show right paratracheal (long arrows), left hilar and subcarinal (short arrows) adenopathy consistent with disease relapse.

19-year-old woman diagnosed with Stage IIA nodular sclerosing Hodgkin’s disease was treated with chemotherapy and 2550 cGy modified mantle irradiation. One year after completing therapy, she developed disease relapse treated with intensive chemotherapy, autologous stem cell rescue and radiation therapy to the lower cervical spine and porta hepatis. A. At diagnosis, the posteroanterior chest radiograph showed right paratracheal adenopathy and bilateral superior mediastinal widening, which improved with therapy. B. By 3-years later, straightening of the left mediastinum and early cephalad retraction of the left hilum is noted. C. Progression of cephalad retraction of the left hilum, coarsening of post-radiation scarring at 11 years, D, from diagnosis are evident and progressed in parallel with decreasing pulmonary function, ultimately leading to her demise.
19-year-old woman diagnosed with Stage IIA nodular sclerosing Hodgkin’s disease was treated with chemotherapy and 2550 cGy modified mantle irradiation. One year after completing therapy, she developed disease relapse treated with intensive chemotherapy, autologous stem cell rescue and radiation therapy to the lower cervical spine and porta hepatis. A. At diagnosis, the posteroanterior chest radiograph showed right paratracheal adenopathy and bilateral superior mediastinal widening, which improved with therapy. B. By 3-years later, straightening of the left mediastinum and early cephalad retraction of the left hilum is noted. C. Progression of cephalad retraction of the left hilum, coarsening of post-radiation scarring at 11 years, D, from diagnosis are evident and progressed in parallel with decreasing pulmonary function, ultimately leading to her demise.

19-year-old woman diagnosed with Stage IIA nodular sclerosing Hodgkin’s disease was treated with chemotherapy and 2550 cGy modified mantle irradiation. One year after completing therapy, she developed disease relapse treated with intensive chemotherapy, autologous stem cell rescue and radiation therapy to the lower cervical spine and porta hepatis. A. At diagnosis, the posteroanterior chest radiograph showed right paratracheal adenopathy and bilateral superior mediastinal widening, which improved with therapy. B. By 3-years later, straightening of the left mediastinum and early cephalad retraction of the left hilum is noted. C. Progression of cephalad retraction of the left hilum, coarsening of post-radiation scarring at 11 years, D, from diagnosis are evident and progressed in parallel with decreasing pulmonary function, ultimately leading to her demise.

This 12-year-old patient was diagnosed with nodular sclerosing Hodgkin’s disease and received multiagent chemotherapy that included anthracycline. Pathologic examination revealed Grade 2 of 3 anthracycline cardiac toxicity. A. Posteroanterior chest radiograph obtained about 1 year after completion of therapy demonstrate cardiomegaly, bilateral pleural effusions and pulmonary vascular congestion indicative of congestive heart failure.

This 49-year-old woman was diagnosed with Wilm’s tumor at age 5 years and received 1200 cGy whole lung irradiation for pulmonary metastases as well as 1200cGy abdominal radiation therapy for primary disease and hepatic metastases. A. and B. A., posteroanterior and lateral, B., chest radiographs demonstrate hypoplasia of both breasts. The anteroposterior diameter of the chest is narrow from radiation-induced rib dysplasia.

This 49-year-old woman was diagnosed with Wilm’s tumor at age 5 years and received 1200 cGy whole lung irradiation for pulmonary metastases as well as 1200cGy abdominal radiation therapy for primary disease and hepatic metastases. A. and B. A., posteroanterior and lateral, B., chest radiographs demonstrate hypoplasia of both breasts. The anteroposterior diameter of the chest is narrow from radiation-induced rib dysplasia.

At the age of 6 years, this boy was diagnosed with Ewings sarcoma family of tumors right chest wall. He received multiagent chemotherapy, surgical resection and 504 cGy external beam irradiation. Over the course of 7 years, he developed significant scoliosis. A. Axial chest computed tomography at the time of diagnosis shows the soft tissue mass arising from the right lateral chest wall. B. Posteroanterior chest radiograph obtained 2 years after completion of therapy show chest wall deformity due to resection of several right thoracic ribs and pulmonary scarring. Note absence of a visible scoliosis. C. Scoliosis series was obtained 7 years after therapy completion due to the presence of a ‘thoracic hump’ demonstrates a 52 degree mid-thoracic rotoscoliosis.

At the age of 6 years, this boy was diagnosed with Ewings sarcoma family of tumors right chest wall. He received multiagent chemotherapy, surgical resection and 504 cGy external beam irradiation. Over the course of 7 years, he developed significant scoliosis. A. Axial chest computed tomography at the time of diagnosis shows the soft tissue mass arising from the right lateral chest wall. B. Posteroanterior chest radiograph obtained 2 years after completion of therapy show chest wall deformity due to resection of several right thoracic ribs and pulmonary scarring. Note absence of a visible scoliosis. C. Scoliosis series was obtained 7 years after therapy completion due to the presence of a ‘thoracic hump’ demonstrates a 52 degree mid-thoracic rotoscoliosis.
At the age of 6 years, this boy was diagnosed with Ewings sarcoma family of tumors right chest wall. He received multiagent chemotherapy, surgical resection and 504 cGy external beam irradiation. Over the course of 7 years, he developed significant scoliosis. A. Axial chest computed tomography at the time of diagnosis shows the soft tissue mass arising from the right lateral chest wall. B. Posteroanterior chest radiograph obtained 2 years after completion of therapy show chest wall deformity due to resection of several right thoracic ribs and pulmonary scarring. Note absence of a visible scoliosis. C. Scoliosis series was obtained 7 years after therapy completion due to the presence of a ‘thoracic hump’ demonstrates a 52 degree mid-thoracic rotoscoliosis.

At the age of 6 years, this boy was diagnosed with Ewings sarcoma family of tumors right chest wall. He received multiagent chemotherapy, surgical resection and 504 cGy external beam irradiation. Over the course of 7 years, he developed significant scoliosis. A. Axial chest computed tomography at the time of diagnosis shows the soft tissue mass arising from the right lateral chest wall. B. Posteroanterior chest radiograph obtained 2 years after completion of therapy show chest wall deformity due to resection of several right thoracic ribs and pulmonary scarring. Note absence of a visible scoliosis. C. Scoliosis series was obtained 7 years after therapy completion due to the presence of a ‘thoracic hump’ demonstrates a 52 degree mid-thoracic rotoscoliosis.

At the age of 6 years, this boy was diagnosed with Ewings sarcoma family of tumors right chest wall. He received multiagent chemotherapy, surgical resection and 504 cGy external beam irradiation. Over the course of 7 years, he developed significant scoliosis. A. Axial chest computed tomography at the time of diagnosis shows the soft tissue mass arising from the right lateral chest wall. B. Posteroanterior chest radiograph obtained 2 years after completion of therapy show chest wall deformity due to resection of several right thoracic ribs and pulmonary scarring. Note absence of a visible scoliosis. C. Scoliosis series was obtained 7 years after therapy completion due to the presence of a ‘thoracic hump’ demonstrates a 52 degree mid-thoracic rotoscoliosis.

This 49-year-old woman was diagnosed with non-Hodgkin’s lymphoma at age 9 years was treated with mediastinal radiation therapy and multiagent chemotherapy. A. and B. A., posteroanterior and lateral, B., chest radiographs demonstrate linear pulmonary scarring with mild cephalad retraction of the hila (arrows), a mild levoconvex mid-thoracic scoliosis (apex of the curve indicated by the arrowhead). The striking chest wall deformity with depression of the anterior chest wall resulted from radiation-induced rib dysplasia. Similarly, note the asymmetric size of the breasts (right smaller than left) and smaller volume of the right hemithorax compared to the left. The lateral view also readily demonstrates demineralization of the thoracic vertebral bodies. C. Posteroanterior chest radiograph at the time of diagnosis show extensive mediastinal, paratracheal and right hilar adenopathy coupled with a large right pleural effusion.

This 49-year-old woman was diagnosed with non-Hodgkin’s lymphoma at age 9 years was treated with mediastinal radiation therapy and multiagent chemotherapy. A. and B. A., posteroanterior and lateral, B., chest radiographs demonstrate linear pulmonary scarring with mild cephalad retraction of the hila (arrows), a mild levoconvex mid-thoracic scoliosis (apex of the curve indicated by the arrowhead). The striking chest wall deformity with depression of the anterior chest wall resulted from radiation-induced rib dysplasia. Similarly, note the asymmetric size of the breasts (right smaller than left) and smaller volume of the right hemithorax compared to the left. The lateral view also readily demonstrates demineralization of the thoracic vertebral bodies. C. Posteroanterior chest radiograph at the time of diagnosis show extensive mediastinal, paratracheal and right hilar adenopathy coupled with a large right pleural effusion.

A 15-year-old boy was diagnosed with Stage IA Hodgkin’s disease of his right neck. In addition to multiagent chemotherapy, treatment included right hemi-mantle irradiation of 1500 cGy. A. Axial computed tomography image of the neck at the time of diagnosis. B. Chest x-ray obtained 15 years after completion of treatment demonstrates asymmetric clavicular growth. The right clavicle measures 2 cm shorter than the left.

A 15-year-old boy was diagnosed with Stage IA Hodgkin’s disease of his right neck. In addition to multiagent chemotherapy, treatment included right hemi-mantle irradiation of 1500 cGy. A. Axial computed tomography image of the neck at the time of diagnosis. B. Chest x-ray obtained 15 years after completion of treatment demonstrates asymmetric clavicular growth. The right clavicle measures 2 cm shorter than the left.

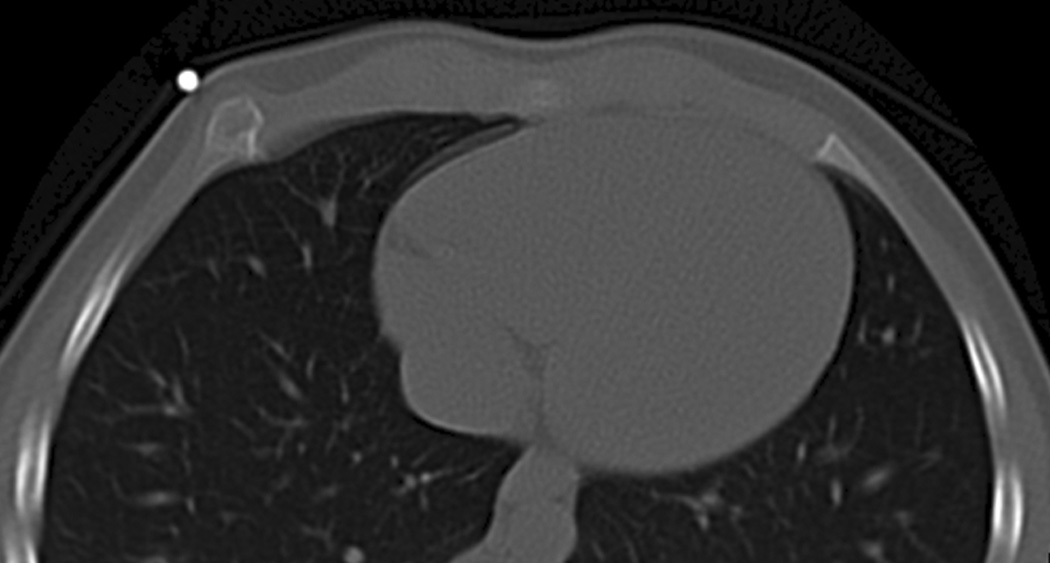
A 7-year-old girl returned 4 years after undergoing bone marrow transplantation for chronic myelogenous leukemia because of a newly found “lump” in her right anterior chest. The preparative regimen for her bone marrow transplantation included total body irradiation. A, posteroanterior chest radiograph was obtained which demonstrated expansion of the right anterior seventh rib (arrow). B. Axial limited chest CT was performed through the rib for characterization of the abnormality shown on the chest radiograph and shows the typical appearance of an exostosis (skin marker).

A 7-year-old girl returned 4 years after undergoing bone marrow transplantation for chronic myelogenous leukemia because of a newly found “lump” in her right anterior chest. The preparative regimen for her bone marrow transplantation included total body irradiation. A, posteroanterior chest radiograph was obtained which demonstrated expansion of the right anterior seventh rib (arrow). B. Axial limited chest CT was performed through the rib for characterization of the abnormality shown on the chest radiograph and shows the typical appearance of an exostosis (skin marker).
A 7-year-old girl returned 4 years after undergoing bone marrow transplantation for chronic myelogenous leukemia because of a newly found “lump” in her right anterior chest. The preparative regimen for her bone marrow transplantation included total body irradiation. A, posteroanterior chest radiograph was obtained which demonstrated expansion of the right anterior seventh rib (arrow). B. Axial limited chest CT was performed through the rib for characterization of the abnormality shown on the chest radiograph and shows the typical appearance of an exostosis (skin marker).

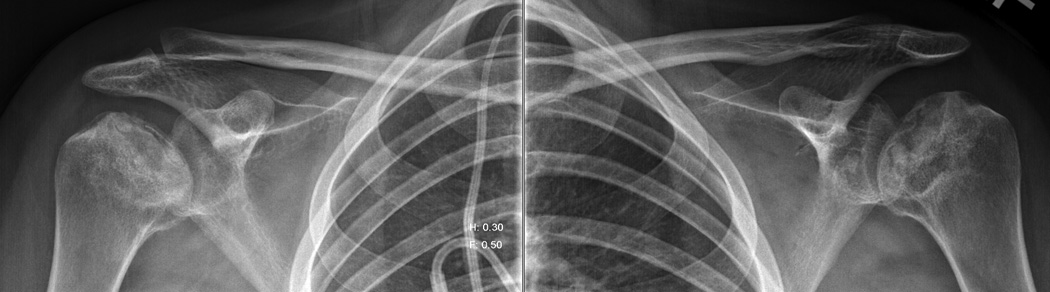
This 20 year-old woman was diagnosed with B-cell non-Hodgkin’s lymphoma at age 16-years and experienced multiple relapses of the disease. She was treated with multiagent chemotherapy that included high dose glucocorticoids. A posteroanterior chest radiograph showed changes of osteonecrosis of the left humeral headA. Dedicated radiographs of the shoulders confirmed the advanced osteonecrotic changes of both humeral heads with crescent signs (arrows), collapse of the articular surfaces, and intermixed areas of sclerosis and cystic changes.
This 20 year-old woman was diagnosed with B-cell non-Hodgkin’s lymphoma at age 16-years and experienced multiple relapses of the disease. She was treated with multiagent chemotherapy that included high dose glucocorticoids. A posteroanterior chest radiograph showed changes of osteonecrosis of the left humeral headA. Dedicated radiographs of the shoulders confirmed the advanced osteonecrotic changes of both humeral heads with crescent signs (arrows), collapse of the articular surfaces, and intermixed areas of sclerosis and cystic changes.
Similar articles
-
Pulmonary outcomes in survivors of childhood central nervous system malignancies: a report from the Childhood Cancer Survivor Study.Pediatr Blood Cancer. 2014 Feb;61(2):319-25. doi: 10.1002/pbc.24819. Epub 2013 Oct 11. Pediatr Blood Cancer. 2014. PMID: 24127436 Free PMC article.
-
Temporal patterns in the risk of chronic health conditions in survivors of childhood cancer diagnosed 1970-99: a report from the Childhood Cancer Survivor Study cohort.Lancet Oncol. 2018 Dec;19(12):1590-1601. doi: 10.1016/S1470-2045(18)30537-0. Epub 2018 Nov 8. Lancet Oncol. 2018. PMID: 30416076 Free PMC article.
-
The EKZ/AMC childhood cancer survivor cohort: methodology, clinical characteristics, and data availability.J Cancer Surviv. 2013 Sep;7(3):439-54. doi: 10.1007/s11764-013-0283-9. Epub 2013 Apr 30. J Cancer Surviv. 2013. PMID: 23625157
-
Second neoplasms in survivors of childhood cancer: findings from the Childhood Cancer Survivor Study cohort.J Clin Oncol. 2009 May 10;27(14):2356-62. doi: 10.1200/JCO.2008.21.1920. Epub 2009 Mar 2. J Clin Oncol. 2009. PMID: 19255307 Free PMC article. Review.
-
Long-term survivors of childhood cancer: the late effects of therapy.Oncologist. 1999;4(1):45-54. Oncologist. 1999. PMID: 10337370 Review.
References
-
- Mariotto AB, Rowland JH, Yabroff KR, et al. Long-term survivors of childhood cancers in the United States. Cancer Epidemiol Biomarkers Prev. 2009;18:1033–1040. - PubMed
-
- Oeffinger KC, Mertens AC, Sklar CA, et al. Chronic health conditions in adult survivors of childhood cancer. N Engl J Med. 2006;355:1572–1582. - PubMed
-
- Friedman DL, Constine LS, Halperin EC, et al. Pediatric Radiation Oncology. Lippincott Williams & Wilkins; 2011. Late Effects of Cancer Treatment; pp. 353–396.
Grants and funding
LinkOut - more resources
Full Text Sources