

Magnetic resonance imaging in acute ischemic stroke treatment
- PMID: 25328872
- PMCID: PMC4200598
- DOI: 10.5853/jos.2014.16.3.131
Magnetic resonance imaging in acute ischemic stroke treatment
Abstract
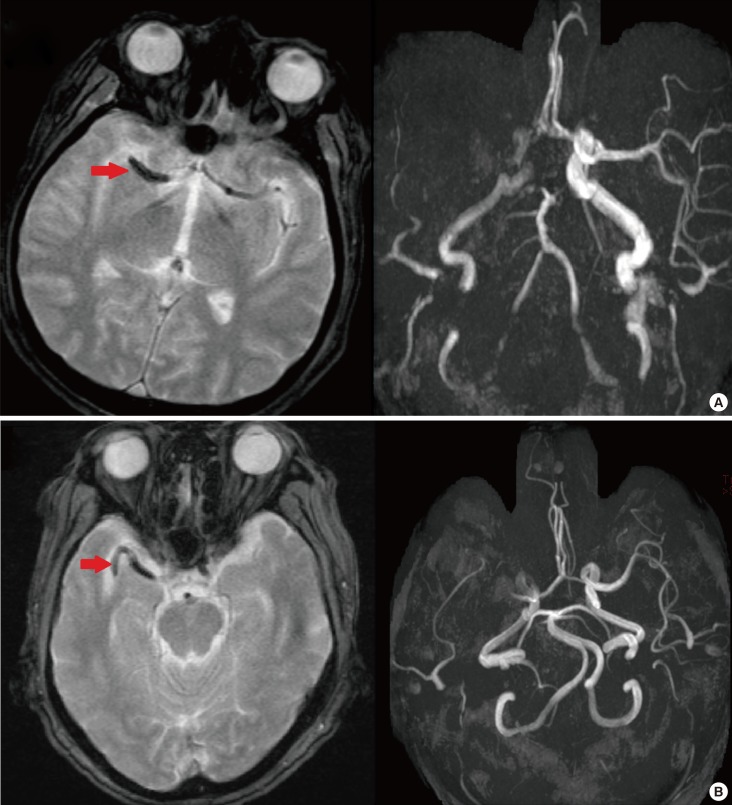
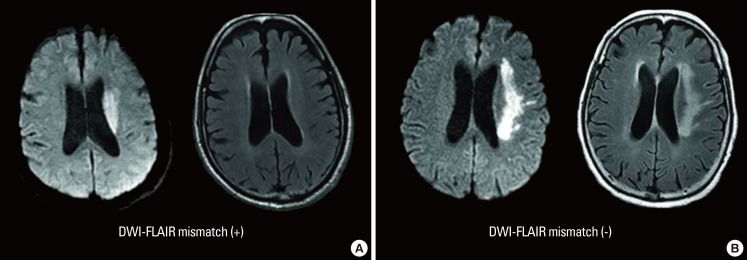
Although intravenous administration of tissue plasminogen activator is the only proven treatment after acute ischemic stroke, there is always a concern of hemorrhagic risk after thrombolysis. Therefore, selection of patients with potential benefits in overcoming potential harms of thrombolysis is of great importance. Despite the practical issues in using magnetic resonance imaging (MRI) for acute stroke treatment, multimodal MRI can provide useful information for accurate diagnosis of stroke, evaluation of the risks and benefits of thrombolysis, and prediction of outcomes. For example, the high sensitivity and specificity of diffusion-weighted image (DWI) can help distinguish acute ischemic stroke from stroke-mimics. Additionally, the lesion mismatch between perfusion-weighted image (PWI) and DWI is thought to represent potential salvageable tissue by reperfusion therapy. However, the optimal threshold to discriminate between benign oligemic areas and the penumbra is still debatable. Signal changes of fluid-attenuated inversion recovery image within DWI lesions may be a surrogate marker for ischemic lesion age and might indicate risks of hemorrhage after thrombolysis. Clot sign on gradient echo image may reflect the nature of clot, and their location, length and morphology may provide predictive information on recanalization by reperfusion therapy. However, previous clinical trials which solely or mainly relied on perfusion-diffusion mismatch for patient selection, failed to show benefits of MRI-based thrombolysis. Therefore, understanding the clinical implication of various useful MRI findings and comprehensively incorporating those variables into therapeutic decision-making may be a more reasonable approach for expanding the indication of acute stroke thrombolysis.
Keywords: Acute ischemic stroke; Magnetic resonance image; Thrombolysis.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures

References
-
- The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. Tissue plasminogen activator for acute ischemic stroke. N Engl J Med. 1995;333:1581–1587. - PubMed
-
- Hacke W, Kaste M, Bluhmki E, Brozman M, Davalos A, Guidetti D, et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med. 2008;359:1317–1329. - PubMed
-
- Khatri R, McKinney AM, Swenson B, Janardhan V. Blood-brain barrier, reperfusion injury, and hemorrhagic transformation in acute ischemic stroke. Neurology. 2012;79:S52–S57. - PubMed
-
- Baird AE, Warach S. Magnetic resonance imaging of acute stroke. J Cereb Blood Flow Metab. 1998;18:583–609. - PubMed
-
- Campbell BC, Tu HT, Christensen S, Desmond PM, Levi CR, Bladin CF, et al. Assessing response to stroke thrombolysis: validation of 24-hour multimodal magnetic resonance imaging. Arch Neurol. 2012;69:46–50. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
