

The role of 18F-FDG PET/CT in large-vessel vasculitis: appropriateness of current classification criteria?
- PMID: 25328890
- PMCID: PMC4190829
- DOI: 10.1155/2014/687608
The role of 18F-FDG PET/CT in large-vessel vasculitis: appropriateness of current classification criteria?
Abstract
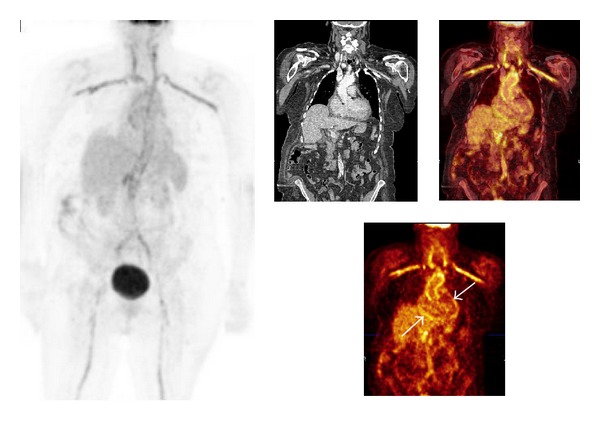
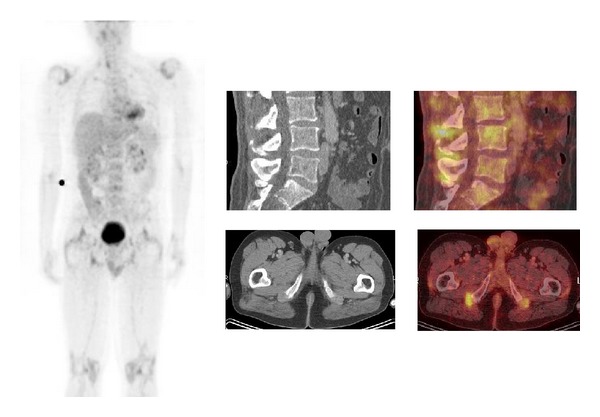
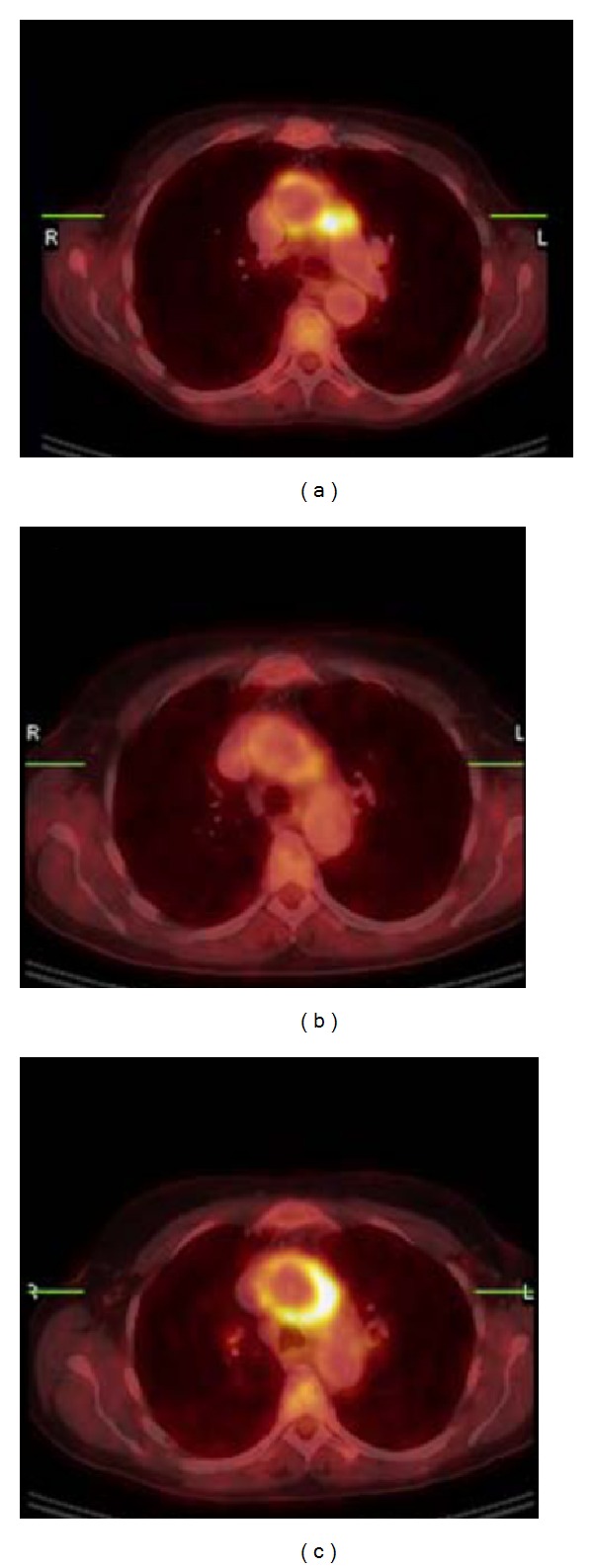
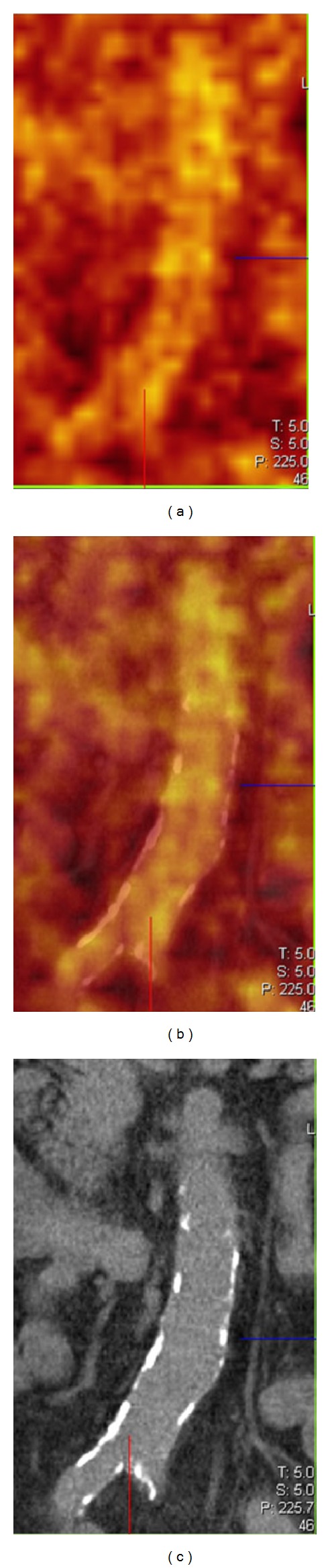
Patients with clinical suspicion of large-vessel vasculitis (LVV) may present with nonspecific signs and symptoms and increased inflammatory parameters and may remain without diagnosis after routine diagnostic procedures. Both the nonspecificity of the radiopharmaceutical (18)F-FDG and the synergy of integrating functional and anatomical images with PET/CT offer substantial benefit in the diagnostic work-up of patients with clinical suspicion for LVV. A negative temporal artery biopsy, an ultrasonography without an arterial halo, or a MRI without aortic wall thickening or oedema do not exclude the presence of LVV and should therefore not exclude the use of (18)F-FDG PET/CT when LVV is clinically suspected. This overview further discusses the notion that there is substantial underdiagnosis of LVV. Late diagnosis of LVV may lead to surgery or angioplasty in occlusive forms and is often accompanied by serious aortic complications and a fatal outcome. In contrast to the American College of Rheumatology 1990 criteria for vasculitis, based on late LVV effects like arterial stenosis and/or occlusion, (18)F-FDG PET/CT sheds new light on the classification of giant cell arteritis (GCA) and Takayasu arteritis (TA). The combination of these observations makes the role of (18)F-FDG PET/CT in the assessment of patients suspected for having LVV promising.
Figures
References
-
- Hunder GG, Arend WP, Bloch DA, et al. The American College of Rheumatology 1990 criteria for the classification of vasculitis: introduction. Arthritis and Rheumatism. 1990;33(8):1065–1067. - PubMed
-
- Arend WP, Michel BA, Bloch DA, et al. The American College of Rheumatology 1990 criteria for the classification of Takayasu arteritis. Arthritis and Rheumatism. 1990;33(8):1129–1134. - PubMed
-
- Hunder GG, Bloch DA, Michel BA, et al. The American College of Rheumatology 1990 criteria for the classification of giant cell arteritis. Arthritis and Rheumatism. 1990;33(8):1122–1128. - PubMed
-
- Jennette JC, Falk RJ, Andrassy K, et al. Nomenclature of systemic vasculitides: proposal of an international consensus conference. Arthritis and Rheumatism. 1994;37(2):187–192. - PubMed
-
- Jennette JC, Falk RJ, Bacon PA, et al. 2012 revised international Chapel Hill consensus conference nomenclature of vasculitides. Arthritis & Rheumatology. 2013;65(1):1–11. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
