

The effect of vestibulo-ocular reflex deficits and covert saccades on dynamic vision in opioid-induced vestibular dysfunction
- PMID: 25329150
- PMCID: PMC4203781
- DOI: 10.1371/journal.pone.0110322
The effect of vestibulo-ocular reflex deficits and covert saccades on dynamic vision in opioid-induced vestibular dysfunction
Abstract
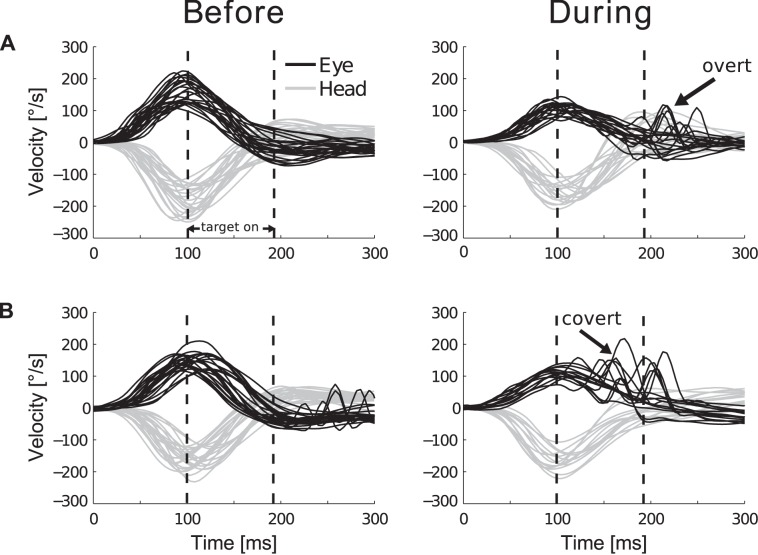
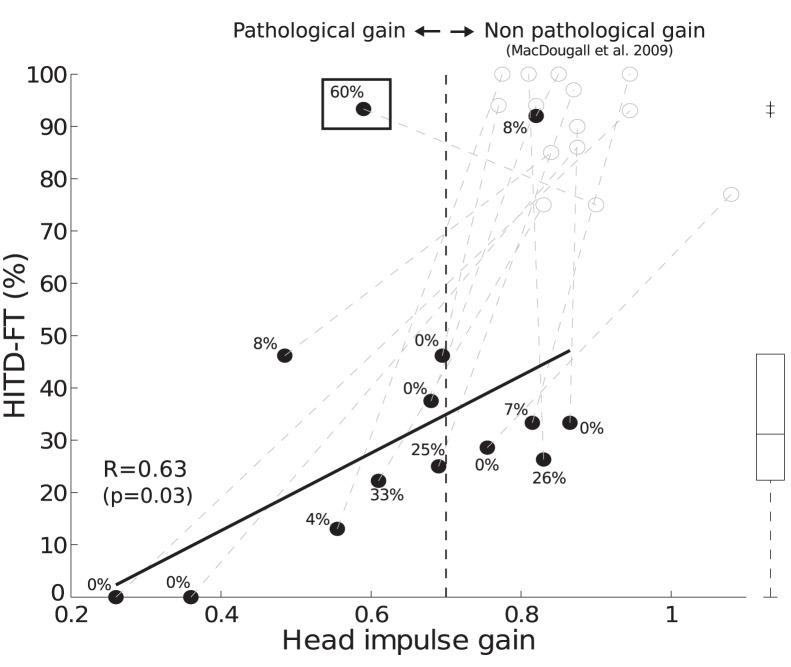
Patients with bilateral vestibular dysfunction cannot fully compensate passive head rotations with eye movements, and experience disturbing oscillopsia. To compensate for the deficient vestibulo-ocular reflex (VOR), they have to rely on re-fixation saccades. Some can trigger "covert" saccades while the head still moves; others only initiate saccades afterwards. Due to their shorter latency, it has been hypothesized that covert saccades are particularly beneficial to improve dynamic visual acuity, reducing oscillopsia. Here, we investigate the combined effect of covert saccades and the VOR on clear vision, using the Head Impulse Testing Device-Functional Test (HITD-FT), which quantifies reading ability during passive high-acceleration head movements. To reversibly decrease VOR function, fourteen healthy men (median age 26 years, range 21-31) were continuously administrated the opioid remifentanil intravenously (0.15 µg/kg/min). VOR gain was assessed with the video head-impulse test, functional performance (i.e. reading) with the HITD-FT. Before opioid application, VOR and dynamic reading were intact (head-impulse gain: 0.87±0.08, mean±SD; HITD-FT rate of correct answers: 90±9%). Remifentanil induced impairment in dynamic reading (HITD-FT 26±15%) in 12/14 subjects, with transient bilateral vestibular dysfunction (head-impulse gain 0.63±0.19). HITD-FT score correlated with head-impulse gain (R = 0.63, p = 0.03) and with gain difference (before/with remifentanil, R = -0.64, p = 0.02). One subject had a non-pathological head-impulse gain (0.82±0.03) and a high HITD-FT score (92%). One subject triggered covert saccades in 60% of the head movements and could read during passive head movements (HITD-FT 93%) despite a pathological head-impulse gain (0.59±0.03) whereas none of the 12 subjects without covert saccades reached such high performance. In summary, early catch-up saccades may improve dynamic visual function. HITD-FT is an appropriate method to assess the combined gaze stabilization effect of both VOR and covert saccades (overall dynamic vision), e.g., to document performance and progress during vestibular rehabilitation.
Conflict of interest statement
Figures
Similar articles
-
Functional Head Impulse Testing Might Be Useful for Assessing Vestibular Compensation After Unilateral Vestibular Loss.Front Neurol. 2018 Nov 19;9:979. doi: 10.3389/fneur.2018.00979. eCollection 2018. Front Neurol. 2018. PMID: 30510538 Free PMC article.
-
Catch-Up Saccades in Vestibulo-Ocular Reflex Deficit: Contribution of Visual Information?Ear Hear. 2025 May-Jun 01;46(3):719-728. doi: 10.1097/AUD.0000000000001616. Epub 2024 Dec 18. Ear Hear. 2025. PMID: 39690450
-
Are Covert Saccade Functionally Relevant in Vestibular Hypofunction?Cerebellum. 2018 Jun;17(3):300-307. doi: 10.1007/s12311-017-0907-0. Cerebellum. 2018. PMID: 29248983 Free PMC article.
-
Video head impulse test: a review of the literature.Eur Arch Otorhinolaryngol. 2017 Mar;274(3):1215-1222. doi: 10.1007/s00405-016-4157-4. Epub 2016 Jun 21. Eur Arch Otorhinolaryngol. 2017. PMID: 27328962 Review.
-
Measure of Central Vestibular Compensation: A Review.J Int Adv Otol. 2022 Sep;18(5):441-446. doi: 10.5152/iao.2022.21207. J Int Adv Otol. 2022. PMID: 35971266 Free PMC article. Review.
Cited by
-
The functional head impulse test: preliminary data.J Neurol. 2018 Oct;265(Suppl 1):35-39. doi: 10.1007/s00415-018-8910-z. Epub 2018 Jun 4. J Neurol. 2018. PMID: 29868981
-
Preventing opioid-induced nausea and vomiting: Rest your head and close your eyes?PLoS One. 2017 Mar 14;12(3):e0173925. doi: 10.1371/journal.pone.0173925. eCollection 2017. PLoS One. 2017. PMID: 28291842 Free PMC article. Clinical Trial.
-
The Effect of Different Head Movement Paradigms on Vestibulo-Ocular Reflex Gain and Saccadic Eye Responses in the Suppression Head Impulse Test in Healthy Adult Volunteers.Front Neurol. 2021 Sep 22;12:729081. doi: 10.3389/fneur.2021.729081. eCollection 2021. Front Neurol. 2021. PMID: 34630303 Free PMC article.
-
Unstable Gaze in Functional Dizziness: A Contribution to Understanding the Pathophysiology of Functional Disorders.Front Neurosci. 2021 Jul 20;15:685590. doi: 10.3389/fnins.2021.685590. eCollection 2021. Front Neurosci. 2021. PMID: 34354560 Free PMC article.
-
New insights into vestibular-saccade interaction based on covert corrective saccades in patients with unilateral vestibular deficits.J Neurophysiol. 2017 Jun 1;117(6):2324-2338. doi: 10.1152/jn.00864.2016. Epub 2017 Apr 12. J Neurophysiol. 2017. PMID: 28404827 Free PMC article.
References
-
- Guinand N, Pijnenburg M, Janssen M, Kingma H (2012) Visual acuity while walking and oscillopsia severity in healthy subjects and patients with unilateral and bilateral vestibular function loss. Arch otolaryngol head neck surg 138: 301–306. - PubMed
-
- Dandy WE (1941) The surgical treatment of Meniere’s disease. Surg Gynecol Obstet 72: 421–425.
-
- Leigh RJ, Averbuch-Heller L, Tomsak RL, Remler BF, Yaniglos SS, et al. (1994) Treatment of abnormal eye movements that impair vision: strategies based on current concepts of physiology and pharmacology. Annals of neurology 36: 129–141. - PubMed
-
- Demer JL, Amjadi F (1993) Dynamic visual acuity of normal subjects during vertical optotype and head motion. Invest Ophthalmol Vis Sci 34: 1894–1906. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
