

Two autopsy cases of severe fever with thrombocytopenia syndrome (SFTS) in Japan: a pathognomonic histological feature and unique complication of SFTS
- PMID: 25329676
- PMCID: PMC4282027
- DOI: 10.1111/pin.12207
Two autopsy cases of severe fever with thrombocytopenia syndrome (SFTS) in Japan: a pathognomonic histological feature and unique complication of SFTS
Abstract
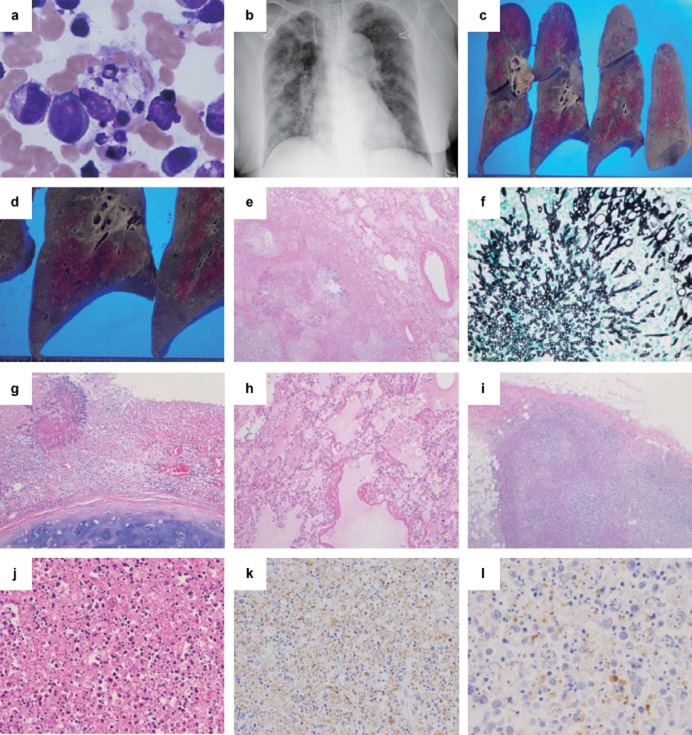
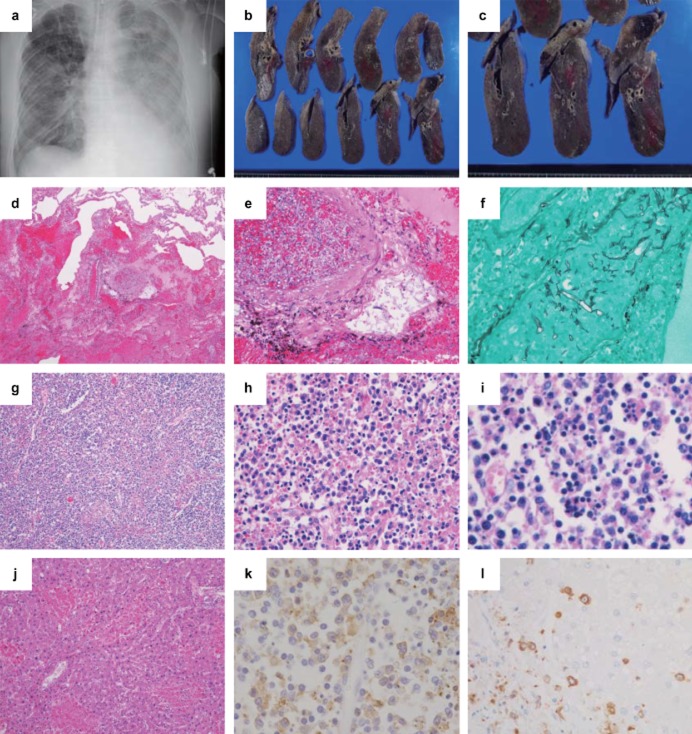
We report two autopsy cases of severe fever with thrombocytopenia syndrome (SFTS) with a high fatality rate in aged Japanese patients. Both cases were caused by a tick-bite. The pathognomonic histological feature was necrotizing lymphadenitis of systemic lymphoid tissue with SFTS viruses and SFTSV-RNA copies. Marked fungal infections were also observed in the lungs of both patients. Since cellular immune function may be suppressed in SFTS patients, physicians should be aware of possible fungal infections.
Keywords: SFTS; SFTS virus-nucleoprotein antigen; autopsy cases; fungal infection; necrotizing lymphadenitis.
© 2014 The Authors. Pathology International published by Japanese Society of Pathology and Wiley Publishing Asia Pty Ltd.
Figures
References
-
- Liu Y, Li Q, Hu W, et al. Person-to-person transmission of severe fever with thrombocytopenia syndrome virus. Vector Borne Zoonotic Dis. 2012;12:156–160. - PubMed
-
- Tang X, Wu W, Wang H, et al. Human-to-human transmission of severe fever with thrombocytopenia syndrome bunyavirus through contact with infectious blood. J Infect Dis. 2013;207:736–739. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
