

Fractional flow reserve: physiological basis, advantages and limitations, and potential gender differences
- PMID: 25329922
- PMCID: PMC4558352
- DOI: 10.2174/1573403x10666141020113318
Fractional flow reserve: physiological basis, advantages and limitations, and potential gender differences
Abstract
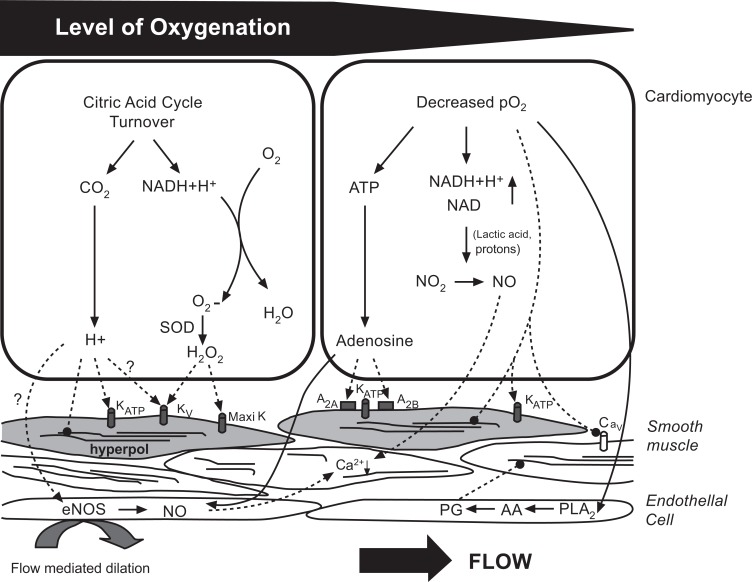
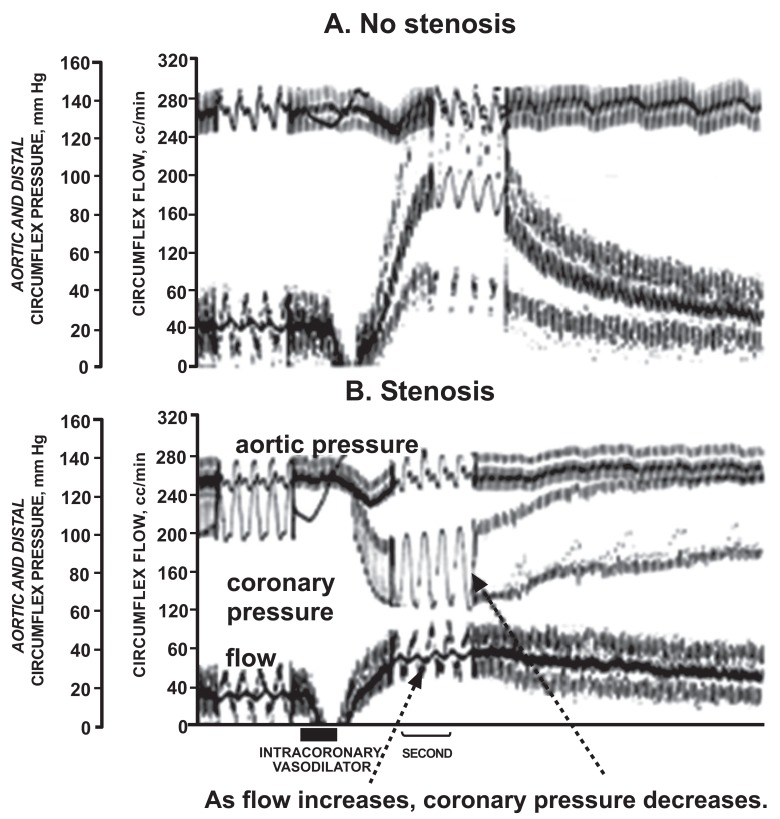
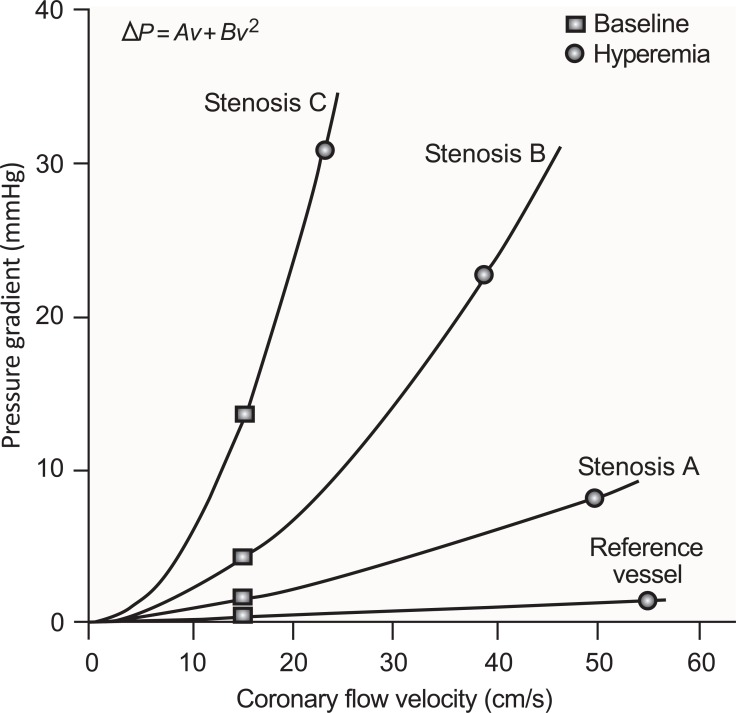
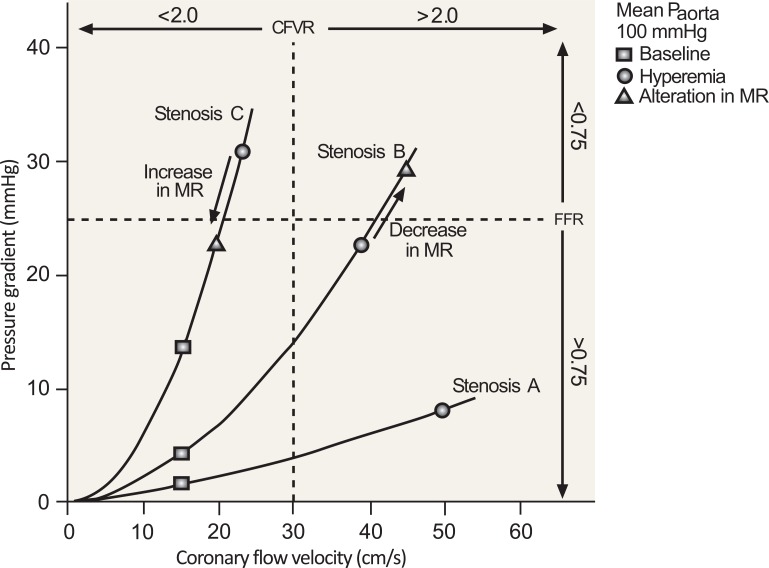
Fractional flow reserve (FFR) is a physiological index of the severity of a stenosis in an epicardial coronary artery, based on the pressure differential across the stenosis. Clinicians are increasingly relying on this method because it is independent of baseline flow, relatively simple, and cost effective. The accurate measurement of FFR is predicated on maximal hyperemia being achieved by pharmacological dilation of the downstream resistance vessels (arterioles). When the stenosis causes FFR to be impaired by > 20%, it is considered to be significant and to justify revascularization. A diminished hyperemic response due to microvascular dysfunction can lead to a false normal FFR value, and a misguided clinical decision. The blunted vasodilation could be the result of defects in the signaling pathways modulated (activated or inhibited) by the drug. This might involve a downregulation or reduced number of vascular receptors, endothelial impairment, or an increased activity of an opposing vasoconstricting mechanism, such as the coronary sympathetic nerves or endothelin. There are data to suggest that microvascular dysfunction is more prevalent in post-menopausal women, perhaps due to reduced estrogen levels. The current review discusses the historical background and physiological basis for FFR, its advantages and limitations, and the phenomenon of microvascular dysfunction and its impact on FFR measurements. The question of whether it is warranted to apply gender-specific guidelines in interpreting FFR measurements is addressed.
Figures
References
-
- Gould K.L., Lipscomb K., Hamilton G.W. Physiologic basis for assessing critical coronary stenosis. Instantaneous flow response and regional distribution during coronary hyperemia as measures of coronary flow reserve. Am. J. Cardiol. 1974;33(1):87–94. doi: 10.1016/0002-9149(74)90743-7. - DOI - PubMed
-
- Pijls N.H., van Son J.A., Kirkeeide R.L., De Bruyne B., Gould K.L. Experimental basis of determining maximum coronary, myocardial, and collateral blood flow by pressure measurements for assessing functional stenosis severity before and after percutaneous transluminal coronary angioplasty. Circulation. 1993;87(4):1354–1367. doi: 10.1161/01.CIR.87.4.1354. - DOI - PubMed
-
- De Bruyne B., Pijls N.H., Paulus W.J., Vantrimpont P.J., Sys S.U., Heyndrickx G.R. Transstenotic coronary pressure gradient measurement in humans: in vitro and in vivo evaluation of a new pressure monitoring angioplasty guide wire. J. Am. Coll. Cardiol. 1993;22(1):119–126. doi: 10.1016/0735-1097(93)90825-L. - DOI - PubMed
-
- Reis S.E., Holubkov R., Lee J.S., Sharaf B., Reichek N., Rogers W.J., Walsh E.G., Fuisz A.R., Kerensky R., Detre K.M., Sopko G., Pepine C.J. Coronary flow velocity response to adenosine characterizes coronary microvascular function in women with chest pain and no obstructive coronary disease. Results from the pilot phase of the Women’s Ischemia Syndrome Evaluation (WISE) study. J. Am. Coll. Cardiol. 1999;33(6):1469–1475. doi: 10.1016/S0735-1097(99)00072-8. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
