

Primary care-based buprenorphine taper vs maintenance therapy for prescription opioid dependence: a randomized clinical trial
- PMID: 25330017
- PMCID: PMC6167926
- DOI: 10.1001/jamainternmed.2014.5302
Primary care-based buprenorphine taper vs maintenance therapy for prescription opioid dependence: a randomized clinical trial
Abstract
Importance: Prescription opioid dependence is increasing and creates a significant public health burden, but primary care physicians lack evidence-based guidelines to decide between tapering doses followed by discontinuation of buprenorphine hydrochloride and naloxone hydrochloride therapy (hereinafter referred to as buprenorphine therapy) or ongoing maintenance therapy.
Objective: To determine the efficacy of buprenorphine taper vs ongoing maintenance therapy in primary care-based treatment for prescription opioid dependence.
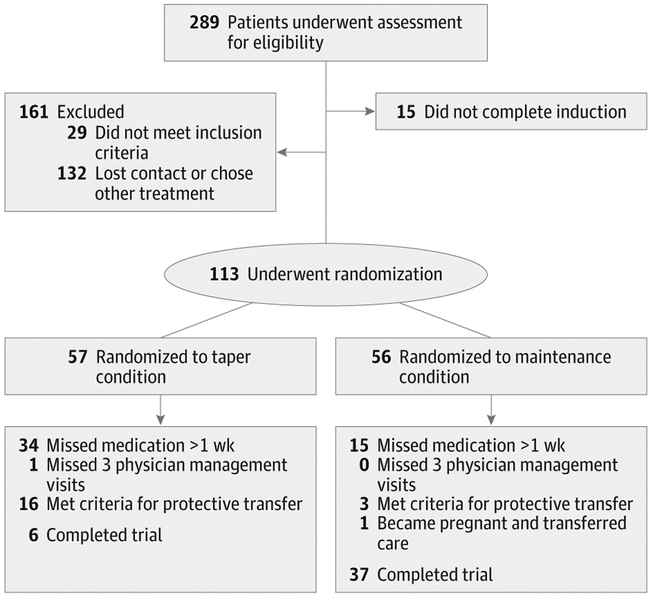
Design, setting, and participants: We conducted a 14-week randomized clinical trial that enrolled 113 patients with prescription opioid dependence from February 17, 2009, through February 1, 2013, in a single primary care site.
Interventions: Patients were randomized to buprenorphine taper (taper condition) or ongoing buprenorphine maintenance therapy (maintenance condition). The buprenorphine taper was initiated after 6 weeks of stabilization, lasted for 3 weeks, and included medications for opioid withdrawal, after which patients were offered naltrexone treatment. The maintenance group received ongoing buprenorphine therapy. All patients received physician and nurse support and drug counseling.
Main outcomes and measures: Illicit opioid use via results of urinanalysis and patient report, treatment retention, and reinitiation of buprenorphine therapy (taper group only).
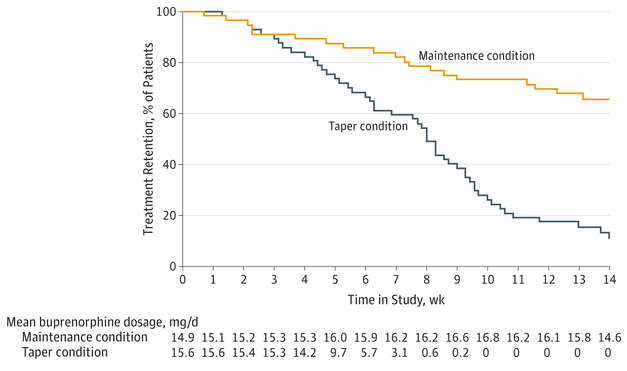
Results: During the trial, the mean percentage of urine samples negative for opioids was lower for patients in the taper group (35.2% [95% CI, 26.2%-44.2%]) compared with those in the maintenance group (53.2% [95% CI, 44.3%-62.0%]). Patients in the taper group reported more days per week of illicit opioid use than those in the maintenance group once they were no longer receiving buprenorphine (mean use, 1.27 [95% CI, 0.60-1.94] vs 0.47 [95% CI, 0.19-0.74] days). Patients in the taper group had fewer maximum consecutive weeks of opioid abstinence compared with those in the maintenance group (mean abstinence, 2.70 [95% CI, 1.72-3.75] vs 5.20 [95% CI, 4.16-6.20] weeks). Patients in the taper group were less likely to complete the trial (6 of 57 [11%] vs 37 of 56 [66%]; P < .001). Sixteen patients in the taper group reinitiated buprenorphine treatment after the taper owing to relapse.
Conclusions and relevance: Tapering is less efficacious than ongoing maintenance treatment in patients with prescription opioid dependence who receive buprenorphine therapy in primary care.
Trial registration: clinicaltrials.gov Identifier: NCT00555425.
Conflict of interest statement
Figures
References
-
- Substance Abuse and Mental Health Services Administration. Results From the 2012 National Survey on Drug Use and Health: Summary of National Findings and Detailed Tables. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2012.
-
- CDC grand rounds: prescription drug overdoses–a US epidemic. Morb Mortal Wkly Rep. 2012;61(1):10–13. - PubMed
-
- Center for Substance Abuse Research. Buprenorphine treatment of opioid dependence. CESAR Fax. 2011;20(34). http://www.cesar.umd.edu/cesar/pubs/BuprenorphineCESARFAX.pdf. Accessed September 4, 2014.
-
- Greene P Outpatient drug utilization trends for buprenorphine years 2002–2009. May 10, 2010. http://buprenorphine.samhsa.gov/bwns/2010_presentations_pdf/09_Greene_50.... Accessed September 4, 2014.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
