

Effects of T-type calcium channel blockers on renal function and aldosterone in patients with hypertension: a systematic review and meta-analysis
- PMID: 25330103
- PMCID: PMC4201480
- DOI: 10.1371/journal.pone.0109834
Effects of T-type calcium channel blockers on renal function and aldosterone in patients with hypertension: a systematic review and meta-analysis
Abstract
Background: High blood pressure can cause kidney damage, which can increase blood pressure, leading to a vicious cycle. It is not clear whether the protective effects of T-type calcium channel blockers (T-type CCBs) on renal function are better than those of L-type CCBs or renin-angiotensin system (RAS) antagonists in patients with hypertension.
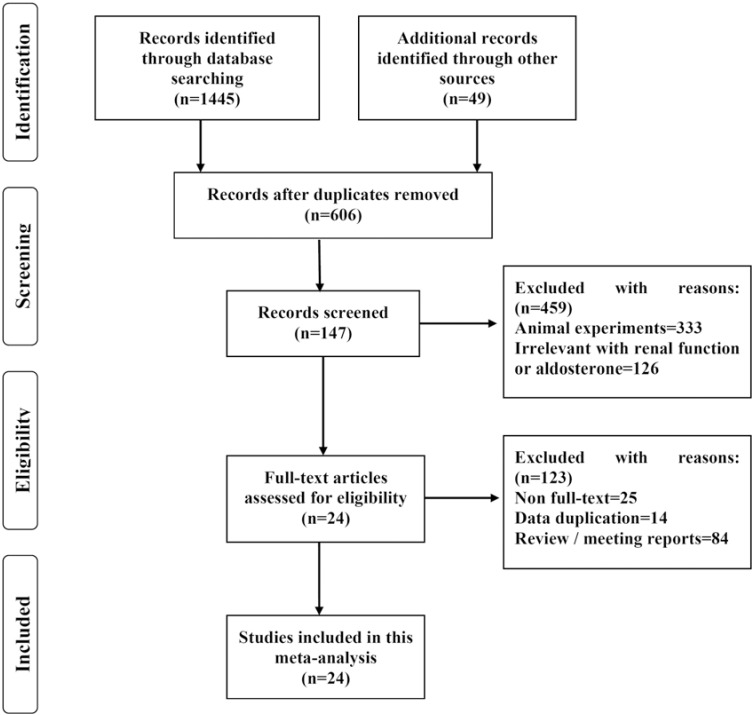
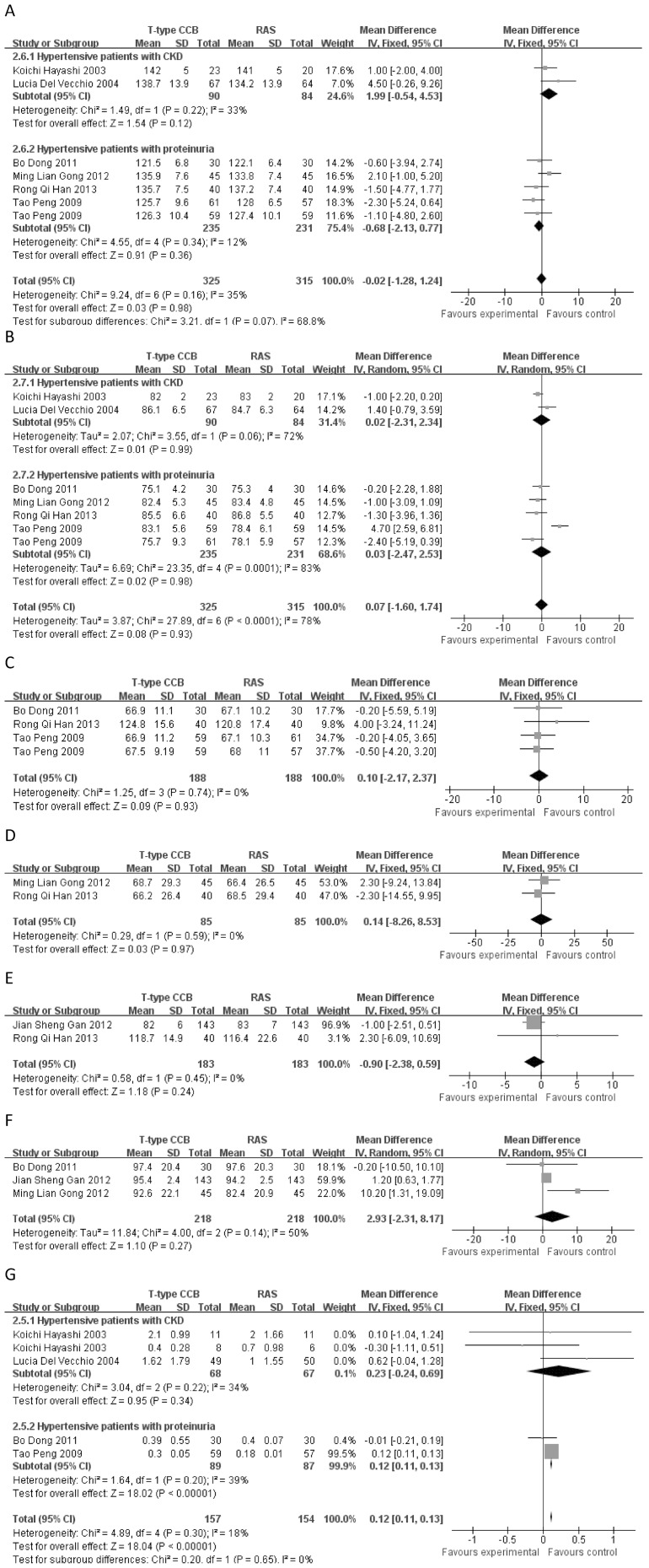
Methods and findings: PUBMED, MEDLINE, EMBASE, OVID, Web of Science, Cochrane, CNKI, MEDCH, VIP, and WANFANG databases were searched for clinical trials published in English or Chinese from January 1, 1990, to December 31, 2013. The weighted mean difference (WMD) and 95% confidence interval (CI) were calculated and reported. A total of 1494 reports were collected, of which 24 studies with 1,696 participants (including 809 reports comparing T-type CCBs versus L-type CCBs and 887 reports comparing T-type CCB versus RAS antagonists) met the inclusion criteria. Compared with L-type CCBs, T-type CCBs resulted in a significant decline in aldosterone (mean difference = -15.19, 95% CI -19.65 - -10.72, p<1×10(-5)), proteinuria (mean difference = -0.73, 95% CI -0.88 - -0.57, p<1×10(-5)), protein to creatinine ratio (mean difference = -0.22, 95% CI -0.41 - -0.03, p = 0.02), and urinary albumin to creatinine ratio (mean difference = -55.38, 95% CI -86.67 - -24.09, p = 0.0005); no significant difference was noted for systolic blood pressure (SBP) (p = 0.76) and diastolic blood pressure (DBP) (p = 0.16). The effects of T-type CCBs did not significantly differ from those of RAS antagonists for SBP (p = 0.98), DBP (p = 0.86), glomerular filtration rate (p = 0.93), albuminuria (p = 0.97), creatinine clearance rate (p = 0.24), and serum creatinine (p = 0.27) in patients with hypertension.
Conclusion: In a pooled analysis of data from 24 studies measuring the effects of T-type CCBs on renal function and aldosterone, the protective effects of T-type CCBs on renal function were enhanced compared with L-type CCBs but did not differ from RAS antagonists. Their protective effects on renal function were independent of blood pressure.
Conflict of interest statement
Figures

Similar articles
-
The effects of calcium channel blockers in the prevention of stroke in adults with hypertension: a meta-analysis of data from 273,543 participants in 31 randomized controlled trials.PLoS One. 2013;8(3):e57854. doi: 10.1371/journal.pone.0057854. Epub 2013 Mar 6. PLoS One. 2013. PMID: 23483932 Free PMC article.
-
Beta-blockers for hypertension.Cochrane Database Syst Rev. 2007 Jan 24;(1):CD002003. doi: 10.1002/14651858.CD002003.pub2. Cochrane Database Syst Rev. 2007. Update in: Cochrane Database Syst Rev. 2012 Aug 15;(8):CD002003. doi: 10.1002/14651858.CD002003.pub3. PMID: 17253471 Updated.
-
Beta-blockers for hypertension.Cochrane Database Syst Rev. 2017 Jan 20;1(1):CD002003. doi: 10.1002/14651858.CD002003.pub5. Cochrane Database Syst Rev. 2017. PMID: 28107561 Free PMC article.
-
Calcium channel blockers for inhibiting preterm labour and birth.Cochrane Database Syst Rev. 2014 Jun 5;2014(6):CD002255. doi: 10.1002/14651858.CD002255.pub2. Cochrane Database Syst Rev. 2014. PMID: 24901312 Free PMC article.
-
Calcium channel blockers for primary and secondary Raynaud's phenomenon.Cochrane Database Syst Rev. 2017 Dec 13;12(12):CD000467. doi: 10.1002/14651858.CD000467.pub2. Cochrane Database Syst Rev. 2017. PMID: 29237099 Free PMC article.
Cited by
-
Calcium channel blocker in patients with chronic kidney disease.Clin Exp Nephrol. 2022 Mar;26(3):207-215. doi: 10.1007/s10157-021-02153-1. Epub 2021 Nov 8. Clin Exp Nephrol. 2022. PMID: 34748113 Free PMC article. Review.
-
Cav 3.2 T-type calcium channel regulates mouse platelet activation and arterial thrombosis.J Thromb Haemost. 2022 Aug;20(8):1887-1899. doi: 10.1111/jth.15745. Epub 2022 May 27. J Thromb Haemost. 2022. PMID: 35490411 Free PMC article.
-
Dihydropyridine calcium channel blockers in the elderly with diabetic nephropathy: Are they safe?J Clin Hypertens (Greenwich). 2018 Jan;20(1):203-204. doi: 10.1111/jch.13158. Epub 2018 Jan 6. J Clin Hypertens (Greenwich). 2018. PMID: 29316147 Free PMC article. No abstract available.
-
Meta-analysis of the efficacy and safety of adding an angiotensin receptor blocker (ARB) to a calcium channel blocker (CCB) following ineffective CCB monotherapy.J Thorac Dis. 2015 Dec;7(12):2243-52. doi: 10.3978/j.issn.2072-1439.2015.12.39. J Thorac Dis. 2015. PMID: 26793346 Free PMC article.
-
Risk factors and urinary biomarkers of non-albuminuric and albuminuric chronic kidney disease in patients with type 2 diabetes.World J Diabetes. 2019 Nov 15;10(11):517-533. doi: 10.4239/wjd.v10.i11.517. World J Diabetes. 2019. PMID: 31798788 Free PMC article.
References
-
- Griffin KA, Picken MM, Bakris GL, Bidani AK (1999) Class differences in the effects of calcium channel blockers in the rat remnant kidney model. Kidney Int 55: 1849–1860. - PubMed
-
- Tomino Y, Shimizu Y, Hamada C, Kurusu A, Ohsawa I, et al. (2011) One-year results of an open-label study on antiproteinuric effect of benidipine in elderly patients with chronic kidney disease. J Nephrol 24: 756–763. - PubMed
-
- Tanaka H, Shigenobu K (2005) Pathophysiological significance of T-type Ca2+ channels: T-type Ca2+ channels and drug development. Pharmacol Sci 99: 214–220. - PubMed
-
- Marin R, Gorostidi M, Fernandez-Vega F, Alvarez-Navascues R (2005) Systemic and glomerular hypertension and progression of chronic renal disease: the dilemma of nephrosclerosis. Kidney Int Suppl 99: 52–56. - PubMed
-
- Wang T, Takabatake T (2005) Effects of vasopeptidase inhibition on renal function and tubuloglomerular feedback in spontaneously hypertensive rats. Hypertens Res 28: 611–618. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
