

Nonmotor symptoms in LRRK2 G2019S associated Parkinson's disease
- PMID: 25330404
- PMCID: PMC4201457
- DOI: 10.1371/journal.pone.0108982
Nonmotor symptoms in LRRK2 G2019S associated Parkinson's disease
Abstract
Background: Idiopathic Parkinson's disease (IPD) and LRRK2-associated PD (LRRK2-PD) might be expected to differ clinically since the neuropathological substrate of LRRK2-PD is heterogeneous. The range and severity of extra-nigral nonmotor features associated with LRRK2 mutations is also not well-defined.
Objective: To evaluate the prevalence and time of onset of nonmotor symptoms (NMS) in LRRK2-PD patients.
Methods: The presence of hyposmia and of neuropsychiatric, dysautonomic and sleep disturbances was assessed in 33 LRRK2-G2019S-PD patients by standardized questionnaires and validated scales. Thirty-three IPD patients, matched for age, gender, duration of parkinsonism and disease severity and 33 healthy subjects were also evaluated.
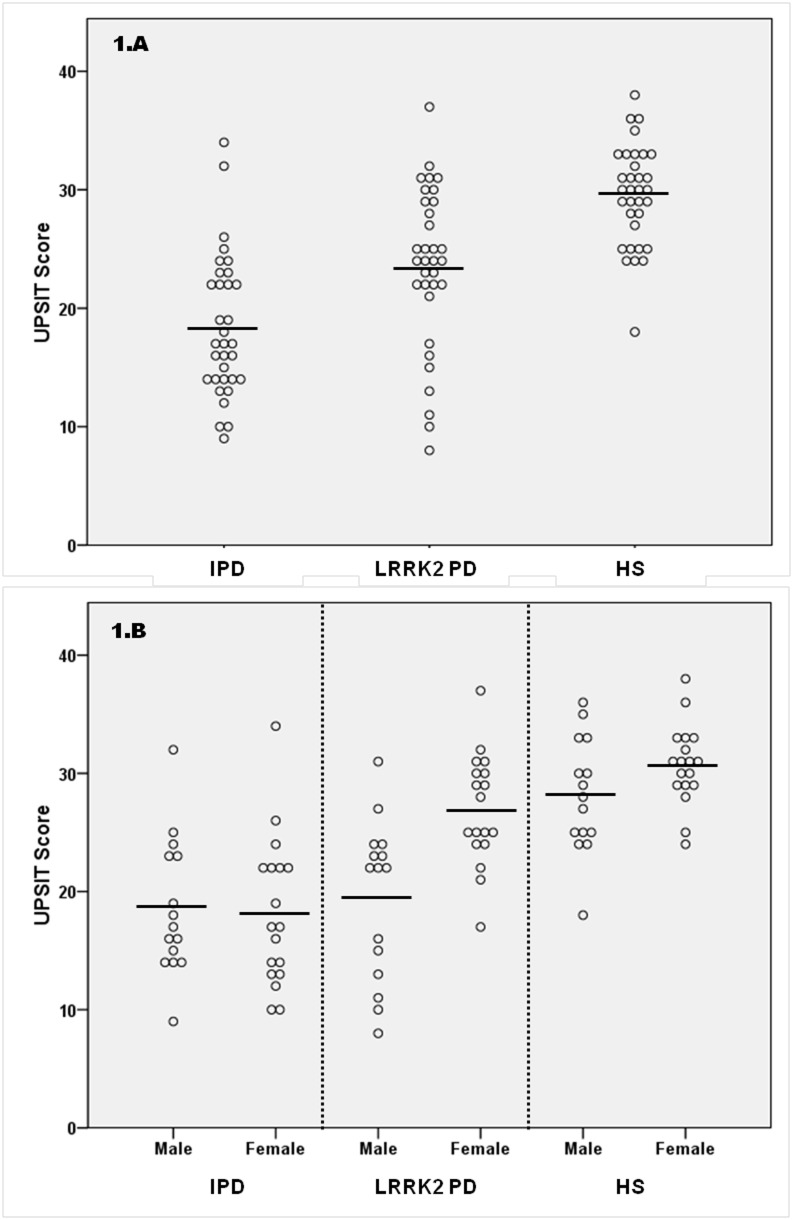
Results: University of Pennsylvania Smell Identification Test (UPSIT) scores in LRRK2-G2019S-PD were higher than those in IPD (23.5±6.8 vs 18.4±6.0; p = 0.002), and hyposmia was less frequent in G2019S carriers than in IPD (39.4% vs 75.8%; p = 0.01). UPSIT scores were significantly higher in females than in males in LRRK2-PD patients (26.9±4.7 vs 19.4±6.8; p<0.01). The frequency of sleep and neuropsychiatric disturbances and of dysautonomic symptoms in LRRK2-G2019S-PD was not significantly different from that in IPD. Hyposmia, depression, constipation and excessive daytime sleepiness, were reported to occur before the onset of classical motor symptoms in more than 40% of LRRK2-PD patients in whom these symptoms were present at the time of examination.
Conclusion: Neuropsychiatric, dysautonomic and sleep disturbances occur as frequently in patients with LRRK2-G2019S-PD as in IPD but smell loss was less frequent in LRRK2-PD. Like in IPD, disturbances such as hyposmia, depression, constipation and excessive daytime sleepiness may antedate the onset of classical motor symptoms in LRRK2-G2019S-PD.
Conflict of interest statement
Figures
References
-
- Paisán Ruíz C, Jain S, Evans EW, Gilks WP, Simón J, et al. (2004) Cloning of the gene containing mutations that cause PARK8-linked Parkinson’s disease. Neuron 44(4): 595–600. - PubMed
-
- Gilks WP, Abou Sleiman PM, Gandhi S, Jain S, Singleton A, et al. (2005) A common LRRK2 mutation in idiopathic Parkinson’s disease. Lancet 365: 415–6. - PubMed
-
- Gaig C, Ezquerra M, Marti MJ, Munoz E, Valldeoriola F, et al. (2006) LRRK2 mutations in Spanish patients with Parkinson disease: frequency, clinical features, and incomplete penetrance. Arch Neurol 63: 377–82. - PubMed
-
- Goldwurm S, Zini M, Di Fonzo A, De Gaspari D, Siri C, et al. (2006) LRRK2 G2019S mutation and Parkinson’s disease: a clinical, neuropsychological and neuropsychiatric study in a large Italian sample. Parkinsonism Relat Disord 12: 410–9. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
