

Novel insights into the biology and treatment of chronic myeloproliferative neoplasms
- PMID: 25330439
- PMCID: PMC5076856
- DOI: 10.3109/10428194.2014.974594
Novel insights into the biology and treatment of chronic myeloproliferative neoplasms
Abstract
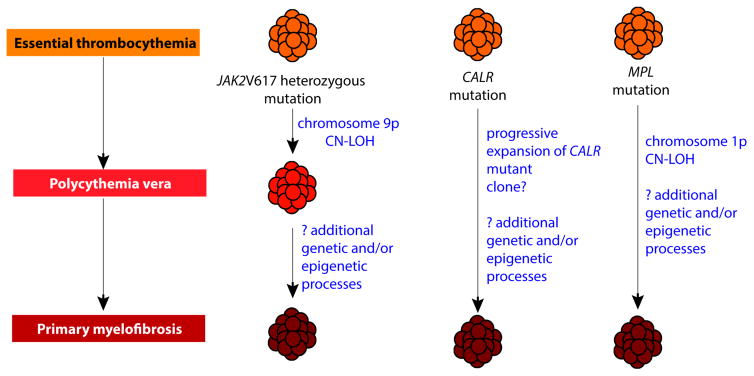
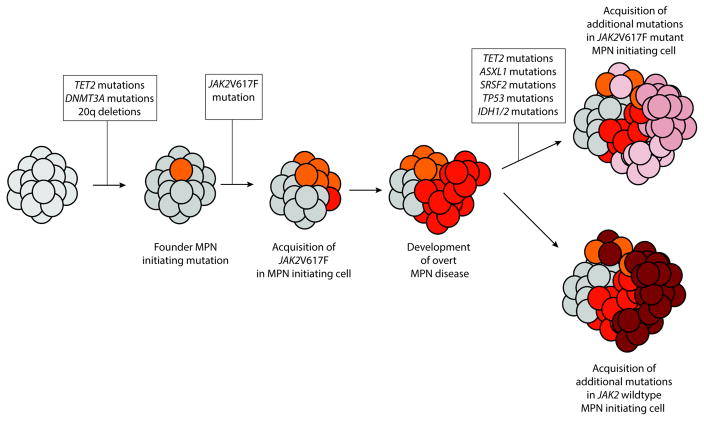
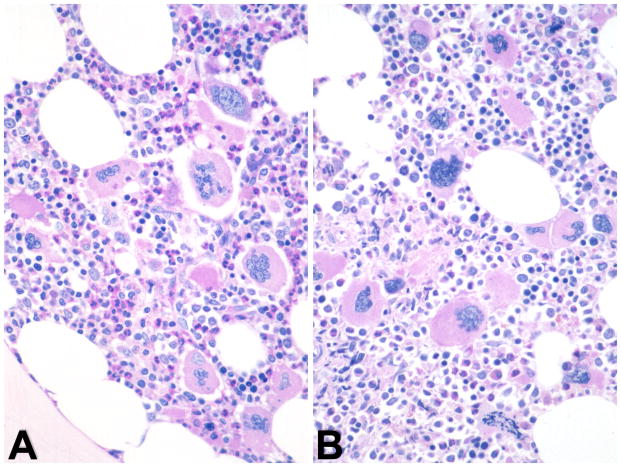
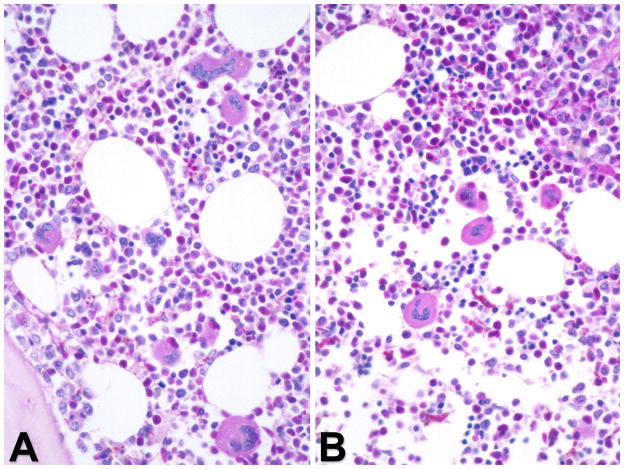
Myeloproliferative neoplasms (MPNs) are clonal disorders of hematopoiesis characterized by a high frequency of genetic alterations, and include chronic myeloid leukemia (CML) and the BCR-ABL1-negative MPNs. Herein we summarize recent advances and controversies in our understanding of the biology and therapy of these disorders, as discussed at the 8th post-American Society of Hematology CML-MPN workshop. The principal areas addressed include the breakthrough discovery of CALR mutations in patients with JAK2/MPL wild type MPN, candidate therapies based on novel genetic findings in leukemic transformation and new therapeutic targets in MPNs, and an appraisal of bone marrow histopathology in MPNs with a focus on the potential new clinical entity of "masked" polycythemia vera. An update on clinical trials of Janus kinase (JAK) inhibitors is presented as well as current understanding regarding the definitions and mechanisms of resistance to JAK inhibitors, and updated information on the safety and efficacy of discontinuation of tyrosine kinase inhibitors in patients with CML.
Keywords: Myeloid leukemias and dysplasias; molecular genetics; myeloproliferative disorders; prognostication; signaling therapies.
Figures

References
-
- Druker B, Talpaz M, Resta DJ, et al. Efficacy and safety of a specific inhibitor of the BCR-ABL tyrosine kinase in chronic myeloid leukemia. N Engl J Med. 2001;344:1031–1042. - PubMed
-
- Cortes J, Hochhaus A, Kim DW, et al. Four-year (yr) follow-up of patients (pts) with newly diagnosed chronic myeloid leukemia in chronic phase (CML-CP) receiving dasatinib or imatinib: efficacy based on early response. Blood. 2013;122(Suppl 1):Abstract 65.
-
- Saglio G, Hochhaus A, Hughes T, et al. ENESTnd update: nilotinib (NIL) vs imatinib (IM) in patients (pts) with newly diagnosed chronic myeloid leukemia in chronic phase (CML-CP) and the impact of early molecular response (EMR) and Sokal risk at diagnosis on long-term outcomes. Blood. 2013;122(Suppl 1):Abstract 92.
-
- James C, Ugo V, Le Couedic JP, et al. A unique clonal JAK2 mutation leading to constitutive signalling causes polycythemia vera. Nature. 2005;434:1144–1148. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous