

Observational study to characterise 24-hour COPD symptoms and their relationship with patient-reported outcomes: results from the ASSESS study
- PMID: 25331383
- PMCID: PMC4220061
- DOI: 10.1186/s12931-014-0122-1
Observational study to characterise 24-hour COPD symptoms and their relationship with patient-reported outcomes: results from the ASSESS study
Abstract
Background: Few studies have investigated the 24-hour symptom profile in patients with COPD or how symptoms during the 24-hour day are inter-related. This observational study assessed the prevalence, severity and relationship between night-time, early morning and daytime COPD symptoms and explored the relationship between 24-hour symptoms and other patient-reported outcomes.
Methods: The study enrolled patients with stable COPD in clinical practice. Baseline night-time, early morning and daytime symptoms (symptom questionnaire), severity of airflow obstruction (FEV1), dyspnoea (modified Medical Research Council Dyspnoea Scale), health status (COPD Assessment Test), anxiety and depression levels (Hospital Anxiety and Depression Scale), sleep quality (COPD and Asthma Sleep Impact Scale) and physical activity level (sedentary, moderately active or active) were recorded.
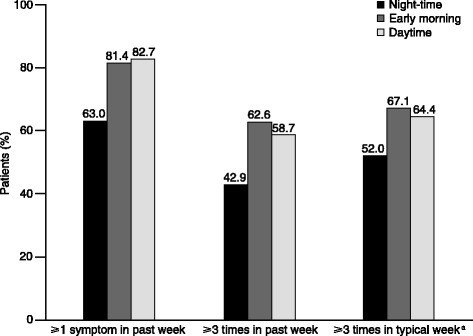
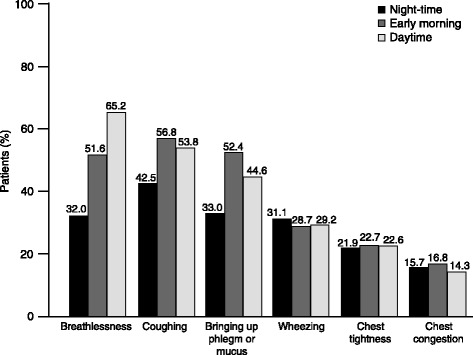
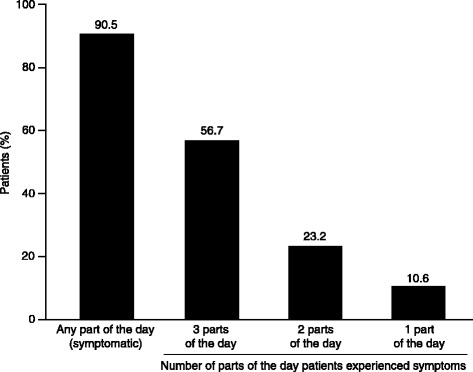
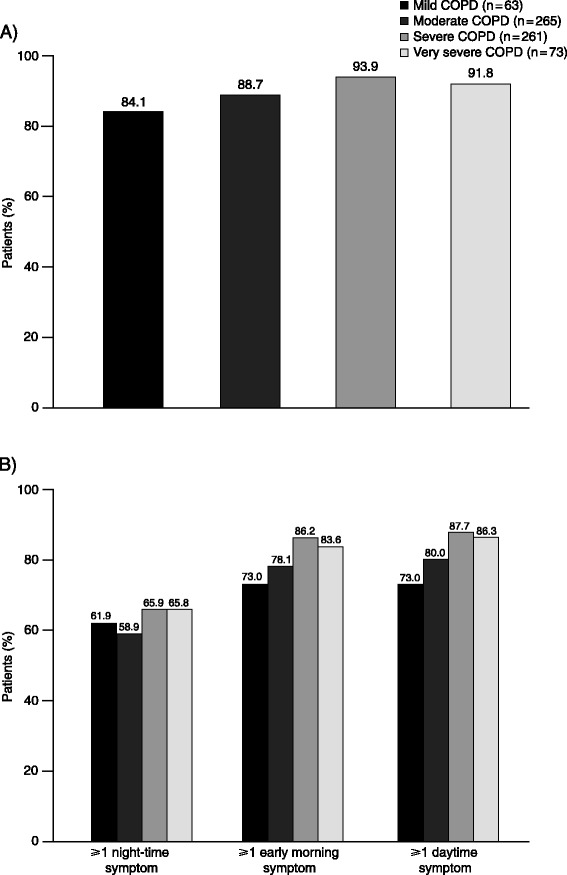
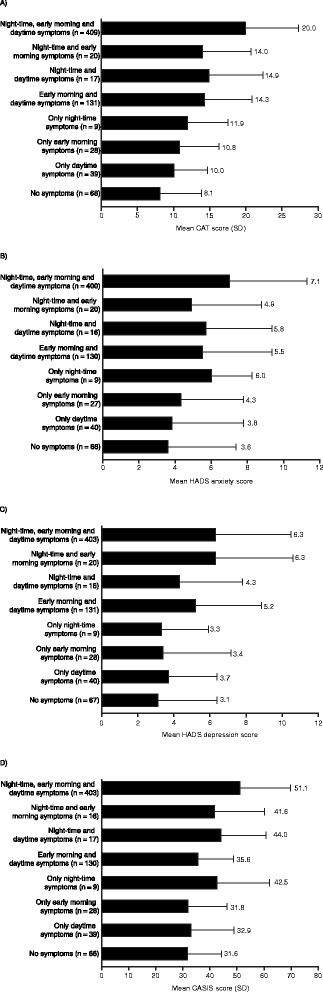
Results: The full analysis set included 727 patients: 65.8% male, mean ± standard deviation age 67.2 ± 8.8 years, % predicted FEV1 52.8 ± 20.5%. In each part of the 24-hour day, >60% of patients reported experiencing ≥1 symptom in the week before baseline. Symptoms were more common in the early morning and daytime versus night-time (81.4%, 82.7% and 63.0%, respectively). Symptom severity was comparable for each period assessed. Overall, in the week before baseline, 56.7% of patients had symptoms throughout the whole 24-hour day (3 parts of the day); 79.9% had symptoms in ≥2 parts of the 24-hour day. Symptoms during each part of the day were inter-related, irrespective of disease severity (all p < 0.001). Early morning and daytime symptoms were associated with the severity of airflow obstruction (p < 0.05 for both). Night-time, early morning and daytime symptoms were all associated with worse dyspnoea, health status and sleep quality, and higher anxiety and depression levels (all p < 0.001 versus patients without symptoms in each corresponding period). In each part of the 24-hour day, there was also an association between symptoms and a patient's physical activity level (p < 0.05 for each period).
Conclusions: More than half of patients experienced COPD symptoms throughout the whole 24-hour day. There was a significant relationship between night-time, early morning and daytime symptoms. In each period, symptoms were associated with worse patient-reported outcomes, suggesting that improving 24-hour symptoms should be an important consideration in the management of COPD.
Figures
Similar articles
-
Circadian rhythm of COPD symptoms in clinically based phenotypes. Results from the STORICO Italian observational study.BMC Pulm Med. 2019 Sep 9;19(1):171. doi: 10.1186/s12890-019-0935-2. BMC Pulm Med. 2019. PMID: 31500607 Free PMC article.
-
The association between objectively measured physical activity and morning symptoms in COPD.Int J Chron Obstruct Pulmon Dis. 2017 Oct 3;12:2831-2840. doi: 10.2147/COPD.S143387. eCollection 2017. Int J Chron Obstruct Pulmon Dis. 2017. PMID: 29042764 Free PMC article.
-
Prevalence and impact of respiratory symptoms in a population of patients with COPD in Latin America: The LASSYC observational study.Respir Med. 2018 Jan;134:62-69. doi: 10.1016/j.rmed.2017.11.018. Epub 2017 Nov 28. Respir Med. 2018. PMID: 29413510
-
Understanding the impact of symptoms on the burden of COPD.Respir Res. 2017 Apr 21;18(1):67. doi: 10.1186/s12931-017-0548-3. Respir Res. 2017. PMID: 28431503 Free PMC article. Review.
-
COPD management: role of symptom assessment in routine clinical practice.Int J Chron Obstruct Pulmon Dis. 2013;8:461-71. doi: 10.2147/COPD.S49392. Epub 2013 Oct 14. Int J Chron Obstruct Pulmon Dis. 2013. PMID: 24143085 Free PMC article. Review.
Cited by
-
The Relationship Between Morning Symptoms and the Risk of Future Exacerbations in COPD.Int J Chron Obstruct Pulmon Dis. 2020 Aug 5;15:1899-1907. doi: 10.2147/COPD.S255030. eCollection 2020. Int J Chron Obstruct Pulmon Dis. 2020. PMID: 32848378 Free PMC article.
-
Nocturnal Dyspnea During Severe Exacerbations Is Associated With Mortality Risk in COPD.Respir Care. 2023 Mar;68(3):413-416. doi: 10.4187/respcare.10310. Epub 2023 Feb 7. Respir Care. 2023. PMID: 36750261 Free PMC article. No abstract available.
-
New developments in optimizing bronchodilator treatment of COPD: a focus on glycopyrrolate/formoterol combination formulated by co-suspension delivery technology.Int J Chron Obstruct Pulmon Dis. 2018 Sep 7;13:2805-2819. doi: 10.2147/COPD.S113306. eCollection 2018. Int J Chron Obstruct Pulmon Dis. 2018. PMID: 30233171 Free PMC article. Review.
-
A Neural Network Approach for Understanding Patient Experiences of Chronic Obstructive Pulmonary Disease (COPD): Retrospective, Cross-sectional Study of Social Media Content.JMIR Med Inform. 2021 Nov 11;9(11):e26272. doi: 10.2196/26272. JMIR Med Inform. 2021. PMID: 34762056 Free PMC article.
-
COPD patients' characteristics, usual care, and adherence to guidelines: the Greek UNLOCK study.Int J Chron Obstruct Pulmon Dis. 2019 Mar 1;14:547-556. doi: 10.2147/COPD.S185362. eCollection 2019. Int J Chron Obstruct Pulmon Dis. 2019. PMID: 30880944 Free PMC article.
References
-
- Tsiligianni I, Kocks J, Tzanakis N, Siafakas N, van der Molen T. Factors that influence disease-specific quality of life or health status in patients with COPD: a review and meta-analysis of Pearson correlations. Prim Care Respir J. 2011;20:257–268. doi: 10.4104/pcrj.2011.00029. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
