

Peripheral CD5+ B cells in antineutrophil cytoplasmic antibody-associated vasculitis
- PMID: 25332071
- PMCID: PMC4497572
- DOI: 10.1002/art.38916
Peripheral CD5+ B cells in antineutrophil cytoplasmic antibody-associated vasculitis
Abstract
Objective: CD5+ B cells have been conceptualized as a possible surrogate for Breg cells. The aim of the present study was to determine the utility of CD5+ B cells as biomarkers in antineutrophil cytoplasmic antibody-associated vasculitis (AAV).
Methods: The absolute and relative numbers (percentages) of CD5+ B cells (explanatory variables) were measured longitudinally during 18 months in 197 patients randomized to receive either rituximab (RTX) or cyclophosphamide (CYC) followed by azathioprine (AZA) for the treatment of AAV (Rituximab in ANCA-Associated Vasculitis [RAVE] trial). Outcome variables included disease activity (status of active disease versus complete remission), responsiveness to induction therapy, disease relapse, disease severity, and, in RTX-treated patients, relapse-free survival according to the percentage of CD5+ B cells detected upon B cell repopulation.
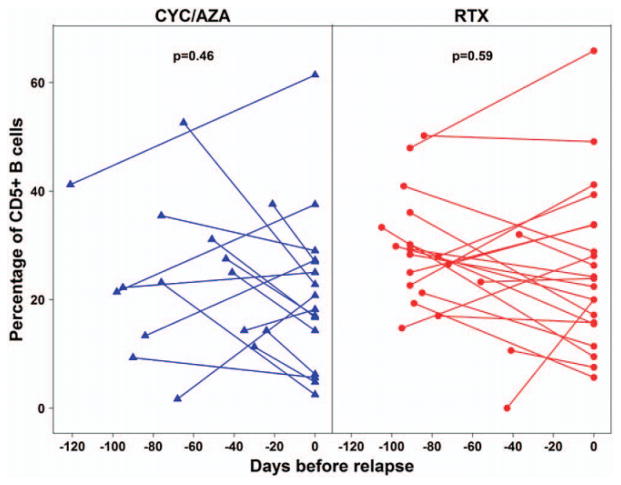
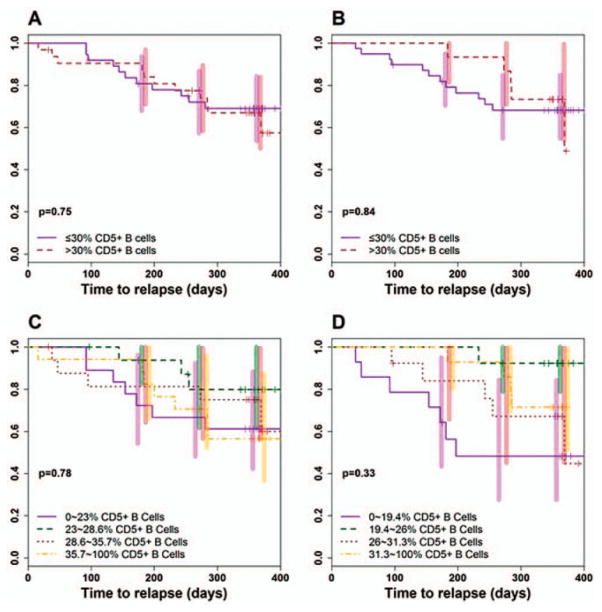
Results: CD5+ B cell numbers were comparable between the treatment groups at baseline. After an initial decline, absolute CD5+ B cell numbers progressively increased in patients in the RTX treatment arm, but remained low in CYC/AZA-treated patients. In both groups, the percentage of CD5+ B cells increased during remission induction and slowly declined thereafter. During relapse, the percentage of CD5+ B cells correlated inversely with disease activity in RTX-treated patients, but not in patients who received CYC/AZA. No significant association was observed between the numbers of CD5+ B cells and induction treatment failure or disease severity. The dynamics of the CD5+ B cell compartment did not anticipate disease relapse. Following B cell repopulation, the percentage of CD5+ B cells was not predictive of time to flare in RTX-treated patients.
Conclusion: The percentage of peripheral CD5+ B cells might reflect disease activity in RTX-treated patients. However, sole staining for CD5 as a putative surrogate marker for Breg cells did not identify a subpopulation of B cells with clear potential for meaningful clinical use. Adequate phenotyping of Breg cells is required to further explore the value of these cells as biomarkers in AAV.
Copyright © 2015 by the American College of Rheumatology.
Figures



References
-
- Dorner T, Radbruch A, Burmester GR. B-cell-directed therapies for autoimmune disease. Nat Rev Rheumatol. 2009;5:433–41. - PubMed
-
- Eming R, Nagel A, Wolff-Franke S, Podstawa E, Debus D, Hertl M. Rituximab exerts a dual effect in pemphigus vulgaris. J Invest Dermatol. 2008;128:2850–8. - PubMed
-
- Mauri C, Bosma A. Immune regulatory function of B cells. Annu Rev Immunol. 2012;30:221–41. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
