

Infrared pupillometry, the Neurological Pupil index and unilateral pupillary dilation after traumatic brain injury: implications for treatment paradigms
- PMID: 25332854
- PMCID: PMC4190183
- DOI: 10.1186/2193-1801-3-548
Infrared pupillometry, the Neurological Pupil index and unilateral pupillary dilation after traumatic brain injury: implications for treatment paradigms
Abstract
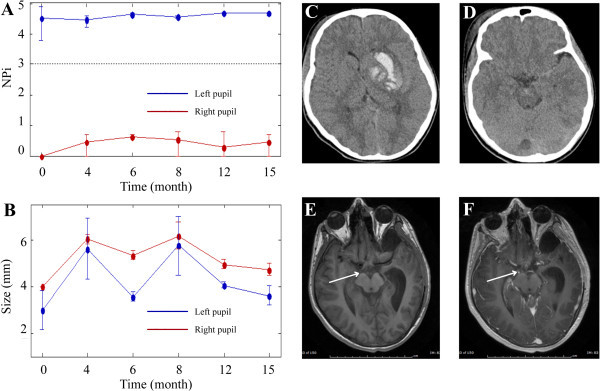
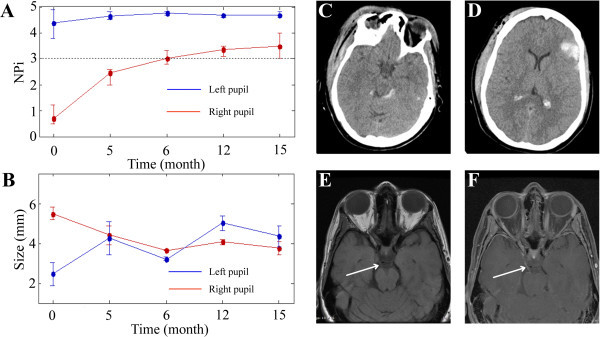
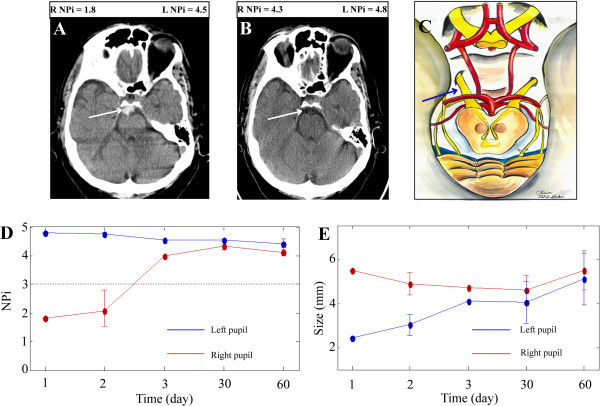
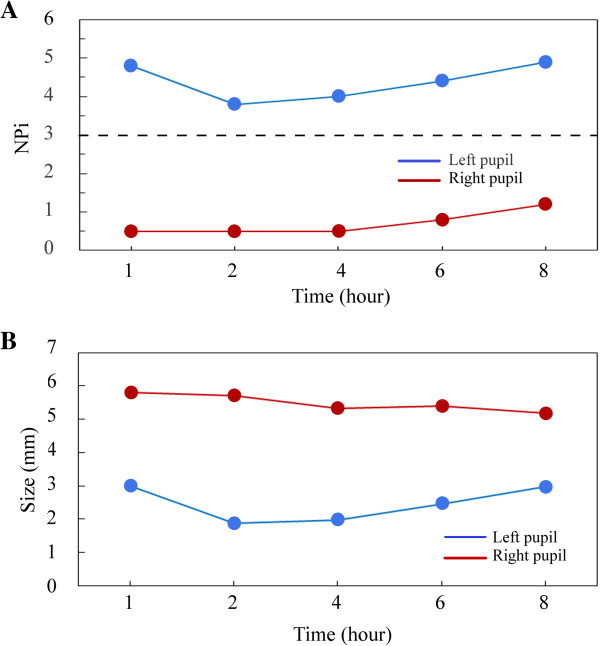
Pupillary dysfunction, a concerning finding in the neurologic examination of the patient with an acute traumatic brain injury often dictates the subsequent treatment paradigm. Patients were monitored closely with an infrared pupillometer, with NPi technology, for acute changes in pupillary function. NPi technology applies a scalar value to pupillary function. A retrospective chart review was performed of traumatic brain injury patients with acute unilateral pupillary dilation, admitted to Legacy Emanuel Medical Center's NeuroTrauma Unit, Portland, OR, and followed as outpatients, between January 2012 and December 2013. Clinical exam findings of pupillary size, NPi scores, and brain Magnetic Resonance Imaging and Computed Tomography images were analyzed. Five traumatic brain injury patients were identified with unilateral pupillary dysfunction with long-term follow-up after the initial injury. Each patient was monitored closely in the trauma bay for neurological deterioration with a pupillometer and the clinical exam. Two patients underwent subsequent intracranial pressure monitoring based on a deteriorating clinical scenario, including consistent abnormal unilateral NPi scores. One patient with consistent abnormal NPi scores and an improved clinical exam did not undergo invasive interventions. Two patients showed early improvement in NPi scores correlating with the normalization of their pupillary reactivity. Anisocoria improved in all patients despite concurrent abnormal NPi scores. Magnetic Resonance Imaging and Computed Tomography imaging studies, with a focus on the third nerve, revealed focal abnormalities consistent with the clinical findings. A unilateral blown pupil and abnormal NPi score in a traumatic brain injury patient are not necessarily indicative of intracranial pressure issues, and must be correlated with the entire clinical scenario, to determine the etiology of the third nerve injury and direct potential therapeutic interventions. Early NPi score normalization suggests pupillary function may improve. We found that NPi scores, as a component of the clinical exam, provide a sensitive, noninvasive and quantitative means of following pupillary function acutely and chronically after a traumatic brain injury.
Keywords: Infrared pupillometry; Neurological Pupil index; Oculomotor nerve palsy; Pupillary outcome; Pupillometer; Traumatic brain injury; Traumatic third nerve palsy.
Figures
References
-
- Boev AN, Fountas KN, Karampelas I, Boev C, Machinis TG, Feltes C, Okosun I, Dimopoulos V, Troup C. Quantitative pupillometry: normative data in healthy pediatric volunteers. J Neurosurg. 2005;103(6 Suppl):496–500. - PubMed
-
- The Brain Trauma Foundation The American Association of Neurological Surgeons. The Joint Section on Neurotrauma and Critical Care. Pupillary diameter and light reflex. J Neurotrauma. 2000;17(6-7):583–590. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
