

Thrombogenic potential of transcatheter aortic valve implantation with trivial paravalvular leakage
- PMID: 25333018
- PMCID: PMC4200687
- DOI: 10.3978/j.issn.2305-5839.2014.05.04
Thrombogenic potential of transcatheter aortic valve implantation with trivial paravalvular leakage
Abstract
Background: Significant paravalvular leakage after transcatheter aortic valve implantation (TAVI) correlates with increased morbidity and mortality, but adverse consequences of trivial paravalvular leakage have stimulated few investigations. Using a unique method distinctly different from other diagnostic approaches, we previously reported elevated backflow velocities of short duration (transients) in mechanical valve closure. In this study, similar transients were found in a transcatheter valve paravalvular leakage avatar.
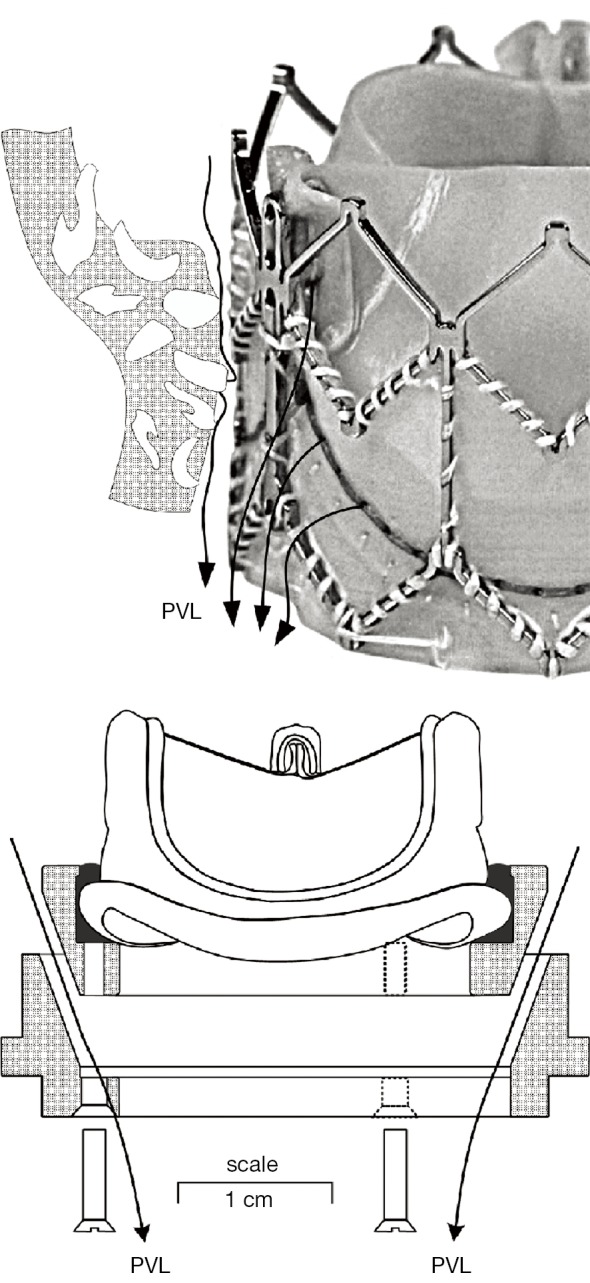
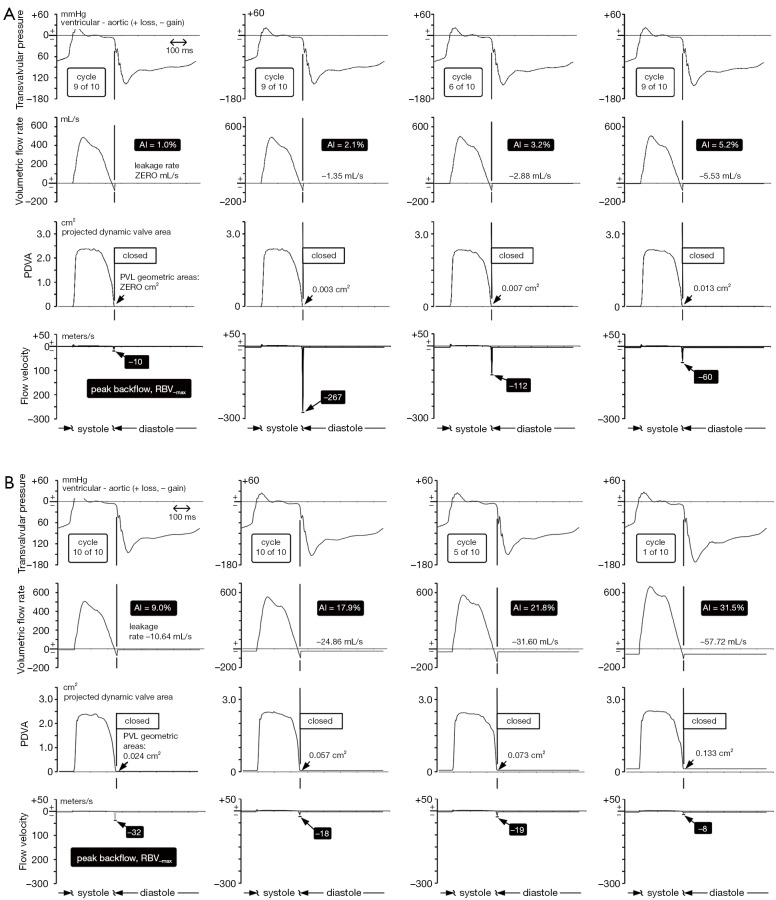
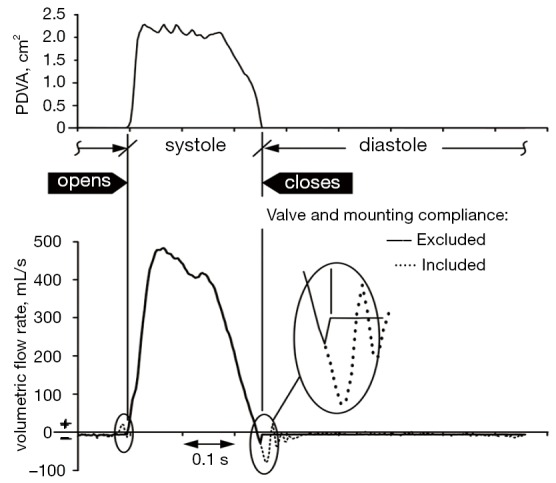
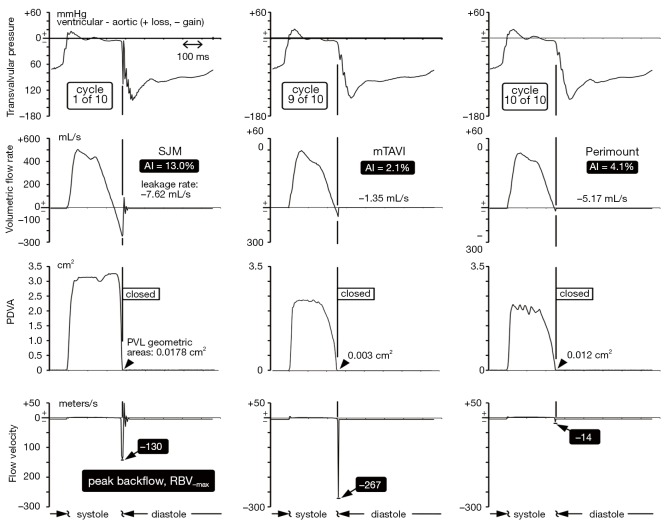
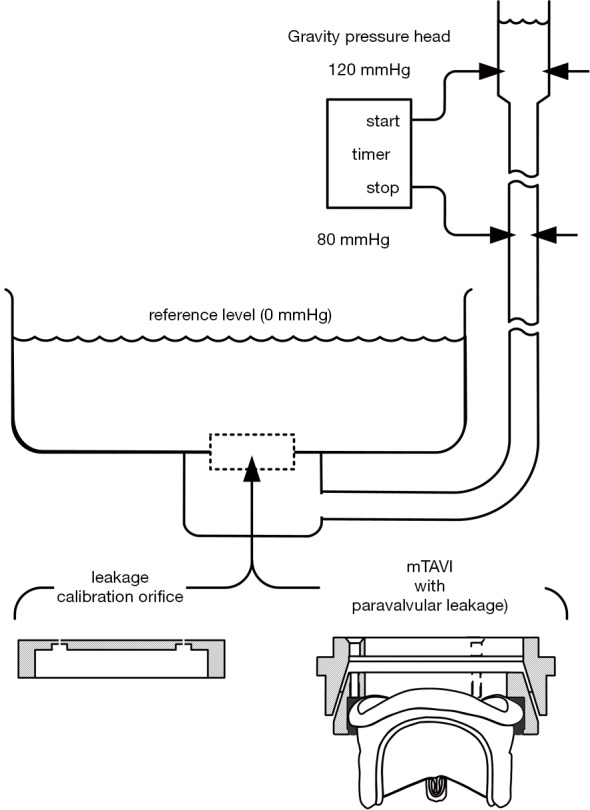
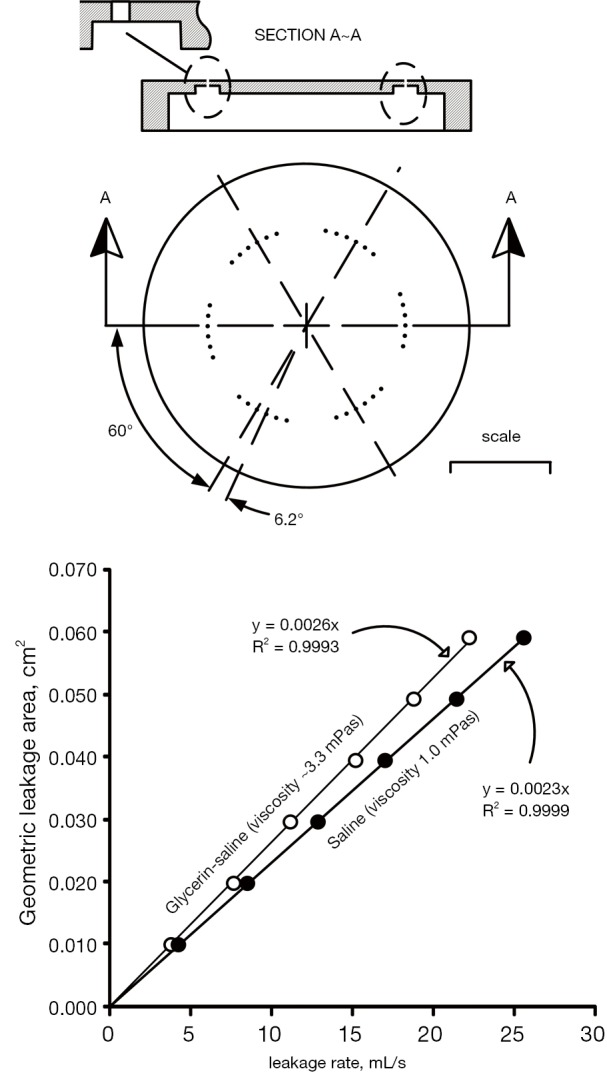
Methods: Paravalvular leakage rate (zero to 58 mL/second) and aortic valve incompetence (volumetric back flow/forward flow; zero to 32%) were made adjustable using a mock transcatheter aortic valve device and tested in quasi-steady and pulsatile flow test systems. Projected dynamic valve area (PDVA) from the back illuminated mock transcatheter aortic valve device was measured and regional backflow velocities were derived by dividing volumetric flow rate by the PDVA over the open and closing valve phase and the total closed valve area derived from backflow leakage.
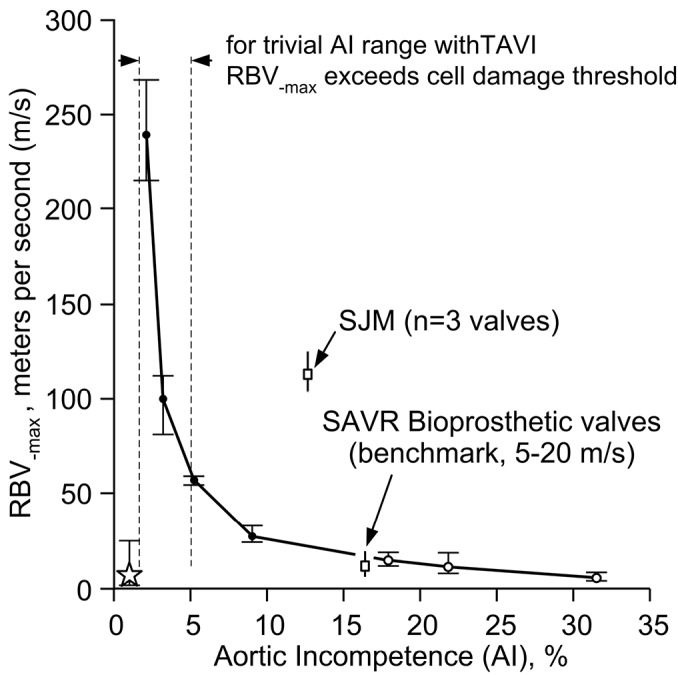
Results: Aortic incompetence from 1-32% generated negative backflow transients from 8 to 267 meters/second, a range not dissimilar to that measured in mechanical valves with zero paravalvular leakage. Optimal paravalvular leakage was identified; not too small generating high backflow transients, not too large considering volume overload and cardiac energy loss caused by defective valve behavior and fluid motion.
Conclusions: Thrombogenic potential of transcatheter aortic valves with trivial aortic incompetence and high magnitude regional backflow velocity transients was comparable to mechanical valves. This may have relevance to stroke rate, asymptomatic microembolic episodes and indications for anticoagulation therapy after transcatheter valve insertion.
Keywords: Transcatheter aortic valve implantation (TAVI); incompetence; leakage; paravalvular; transients.
Figures
Similar articles
-
Importance of shear in prosthetic valve closure dynamics.J Heart Valve Dis. 2011 Nov;20(6):664-72. J Heart Valve Dis. 2011. PMID: 22655497
-
Transapical aortic valve implantation: incidence and predictors of paravalvular leakage and transvalvular regurgitation in a series of 358 patients.J Am Coll Cardiol. 2012 Jan 17;59(3):211-21. doi: 10.1016/j.jacc.2011.10.857. J Am Coll Cardiol. 2012. PMID: 22240125
-
Are anticoagulant independent mechanical valves within reach-fast prototype fabrication and in vitro testing of innovative bi-leaflet valve models.Ann Transl Med. 2015 Aug;3(14):197. doi: 10.3978/j.issn.2305-5839.2015.08.18. Ann Transl Med. 2015. PMID: 26417581 Free PMC article.
-
Next-generation transcatheter heart valves: current trials in Europe and the USA.Methodist Debakey Cardiovasc J. 2012 Apr-Jun;8(2):9-12. doi: 10.14797/mdcj-8-2-9. Methodist Debakey Cardiovasc J. 2012. PMID: 22891121 Free PMC article. Review.
-
Impact of paravalvular aortic regurgitation after transcatheter aortic valve implantation on survival.Int J Cardiol. 2016 Oct 15;221:46-51. doi: 10.1016/j.ijcard.2016.07.006. Epub 2016 Jul 4. Int J Cardiol. 2016. PMID: 27400296 Review.
Cited by
-
Principles of TAVR valve design, modelling, and testing.Expert Rev Med Devices. 2018 Nov;15(11):771-791. doi: 10.1080/17434440.2018.1536427. Epub 2018 Oct 29. Expert Rev Med Devices. 2018. PMID: 30318937 Free PMC article. Review.
-
Clinical predictors and sequelae of computed tomography defined leaflet thrombosis following transcatheter aortic valve replacement at medium-term follow-up.Heart Vessels. 2021 Sep;36(9):1374-1383. doi: 10.1007/s00380-021-01803-4. Epub 2021 Mar 4. Heart Vessels. 2021. PMID: 33660057
-
Prosthetic Aortic Valves: Challenges and Solutions.Front Cardiovasc Med. 2018 May 14;5:46. doi: 10.3389/fcvm.2018.00046. eCollection 2018. Front Cardiovasc Med. 2018. PMID: 29868612 Free PMC article.
-
Patient-specific simulation of transcatheter aortic valve replacement: impact of deployment options on paravalvular leakage.Biomech Model Mechanobiol. 2019 Apr;18(2):435-451. doi: 10.1007/s10237-018-1094-8. Epub 2018 Nov 20. Biomech Model Mechanobiol. 2019. PMID: 30460623 Free PMC article.
-
New Insights into Valve Hemodynamics.Rambam Maimonides Med J. 2020 Apr 29;11(2):e0014. doi: 10.5041/RMMJ.10400. Rambam Maimonides Med J. 2020. PMID: 32374253 Free PMC article. Review.
References
-
- Cribier A, Eltchaninoff H, Bash A, et al. Percutaneous transcatheter implantation of an aortic valve prosthesis for calcific aortic stenosis: first human case description. Circulation 2002;106:3006-8. - PubMed
-
- Cribier A.Perspective on transcatheter aortic valve implantation: past, present, and future. Chin Med J (Engl) 2013;126:1008-12. - PubMed
-
- Sponga S, Perron J, Dagenais F, et al. Impact of residual regurgitation after aortic valve replacement. Eur J Cardiothorac Surg 2012;42:486-92. - PubMed
-
- Gripari P, Ewe SH, Fusini L, et al. Intraoperative 2D and 3D transoesophageal echocardiographic predictors of aortic regurgitation after transcatheter aortic valve implantation. Heart 2012;98:1229-36. - PubMed
LinkOut - more resources
Full Text Sources