

Low-frequency drug-resistant HIV-1 and risk of virological failure to first-line NNRTI-based ART: a multicohort European case-control study using centralized ultrasensitive 454 pyrosequencing
- PMID: 25336166
- PMCID: PMC4319483
- DOI: 10.1093/jac/dku426
Low-frequency drug-resistant HIV-1 and risk of virological failure to first-line NNRTI-based ART: a multicohort European case-control study using centralized ultrasensitive 454 pyrosequencing
Abstract
Objectives: It is still debated if pre-existing minority drug-resistant HIV-1 variants (MVs) affect the virological outcomes of first-line NNRTI-containing ART.
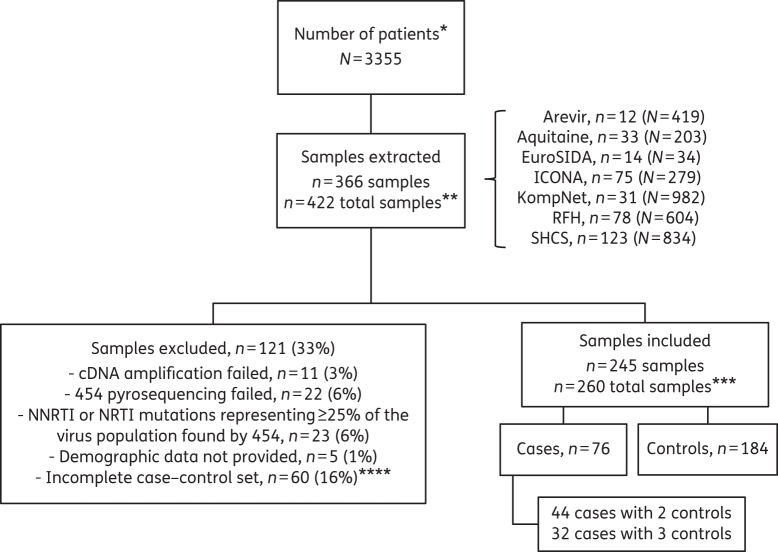
Methods: This Europe-wide case-control study included ART-naive subjects infected with drug-susceptible HIV-1 as revealed by population sequencing, who achieved virological suppression on first-line ART including one NNRTI. Cases experienced virological failure and controls were subjects from the same cohort whose viraemia remained suppressed at a matched time since initiation of ART. Blinded, centralized 454 pyrosequencing with parallel bioinformatic analysis in two laboratories was used to identify MVs in the 1%-25% frequency range. ORs of virological failure according to MV detection were estimated by logistic regression.
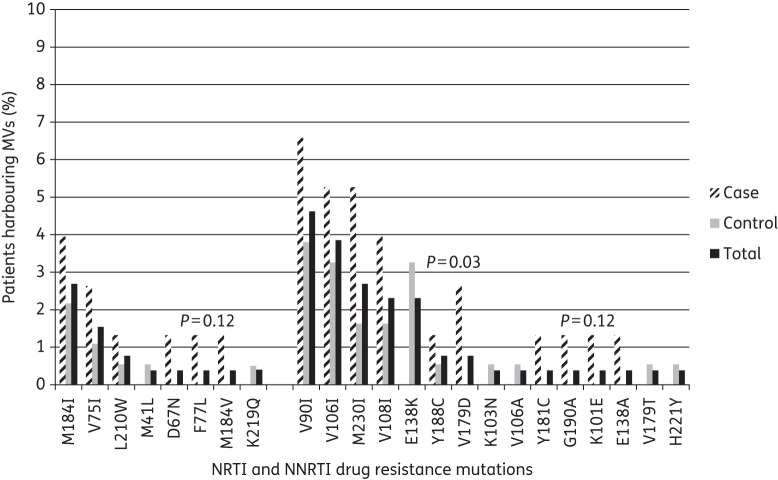
Results: Two hundred and sixty samples (76 cases and 184 controls), mostly subtype B (73.5%), were used for the analysis. Identical MVs were detected in the two laboratories. 31.6% of cases and 16.8% of controls harboured pre-existing MVs. Detection of at least one MV versus no MVs was associated with an increased risk of virological failure (OR = 2.75, 95% CI = 1.35-5.60, P = 0.005); similar associations were observed for at least one MV versus no NRTI MVs (OR = 2.27, 95% CI = 0.76-6.77, P = 0.140) and at least one MV versus no NNRTI MVs (OR = 2.41, 95% CI = 1.12-5.18, P = 0.024). A dose-effect relationship between virological failure and mutational load was found.
Conclusions: Pre-existing MVs more than double the risk of virological failure to first-line NNRTI-based ART.
Keywords: CHAIN; European multicentre study; antiretroviral therapy; minority drug-resistant HIV-1 variants.
© The Author 2014. Published by Oxford University Press on behalf of the British Society for Antimicrobial Chemotherapy.
Figures
References
-
- WHO. HIV Drug Resistance Report 2012. http://www.who.int/hiv/pub/drugresistance/report2012/en/
-
- Gilks CF, Crowley S, Ekpini R, et al. The WHO public-health approach to antiretroviral treatment against HIV in resource-limited settings. Lancet. 2006;368:505–10. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
