

Small cell lung cancer: where do we go from here?
- PMID: 25336398
- PMCID: PMC5497465
- DOI: 10.1002/cncr.29098
Small cell lung cancer: where do we go from here?
Abstract
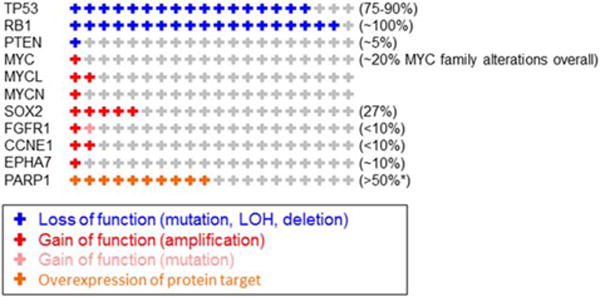
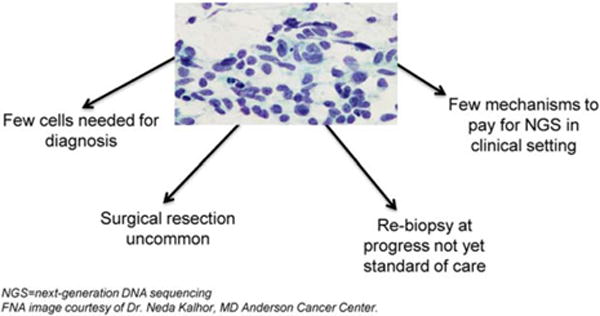
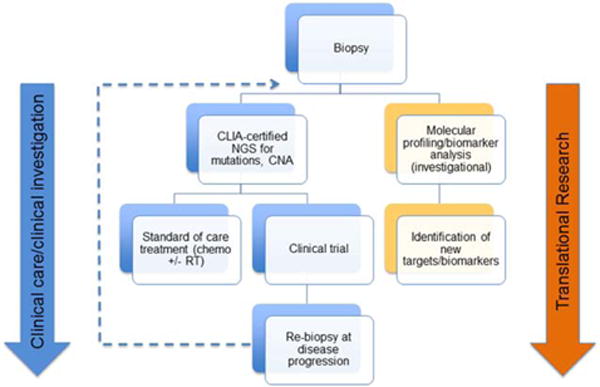
Small cell lung cancer (SCLC) is an aggressive disease that accounts for approximately 14% of all lung cancers. In the United States, approximately 31,000 patients are diagnosed annually with SCLC. Despite numerous clinical trials, including at least 40 phase 3 trials since the 1970s, systemic treatment for patients with SCLC has not changed significantly in the past several decades. Consequently, the 5-year survival rate remains low at <7% overall, and most patients survive for only 1 year or less after diagnosis. Unlike nonsmall cell lung cancer (NSCLC), in which major advances have been made using targeted therapies, there are still no approved targeted drugs for SCLC. Significant barriers to progress in SCLC include 1) a lack of early detection modalities, 2) limited tumor tissue for translational research (eg, molecular profiling of DNA, RNA, and/or protein alterations) because of small diagnostic biopsies and the rare use of surgical resection in standard treatment, and 3) rapid disease progression with poor understanding of the mechanisms contributing to therapeutic resistance. In this report, the authors review the current state of SCLC treatment, recent advances in current understanding of the underlying disease biology, and opportunities to advance translational research and therapeutic approaches for patients with SCLC.
Keywords: genomics; novel therapies; proteomics; small cell lung cancer; translational research.
© 2014 American Cancer Society.
Conflict of interest statement
CONFLICT OF INTEREST DISCLOSURES
Dr. Byers reports consulting fees from BioMarin and AbbVie outside the submitted work. Dr. Rudin reports consulting fees from AbbVie, Aveo/Biodesik, Boehringer Ingelheim, GlaxoSmithKline, and Merck outside the submitted work.
Figures
References
-
- American Cancer Society. Cancer Facts & Figures 2014. Atlanta, GA: American Cancer Society; 2014.
-
- Ettinger DS, Aisner J. Changing face of small-cell lung cancer: real and artifact. J Clin Oncol. 2006;24:4526–4527. - PubMed
-
- Miller CW, Simon K, Aslo A, et al. p53 mutations in human lung tumors. Cancer Res. 1992;52:1695–1698. - PubMed
-
- Takahashi T, Suzuki H, Hida T, Sekido Y, Ariyoshi Y, Ueda R. The p53 gene is very frequently mutated in small-cell lung cancer with a distinct nucleotide substitution pattern. Oncogene. 1991;6:1775–1778. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
