

Brain edema predicts outcome after nonlacunar ischemic stroke
- PMID: 25336512
- PMCID: PMC4295905
- DOI: 10.1161/STROKEAHA.114.006884
Brain edema predicts outcome after nonlacunar ischemic stroke
Abstract
Background and purpose: In malignant infarction, brain edema leads to secondary neurological deterioration and poor outcome. We sought to determine whether swelling is associated with outcome in smaller volume strokes.
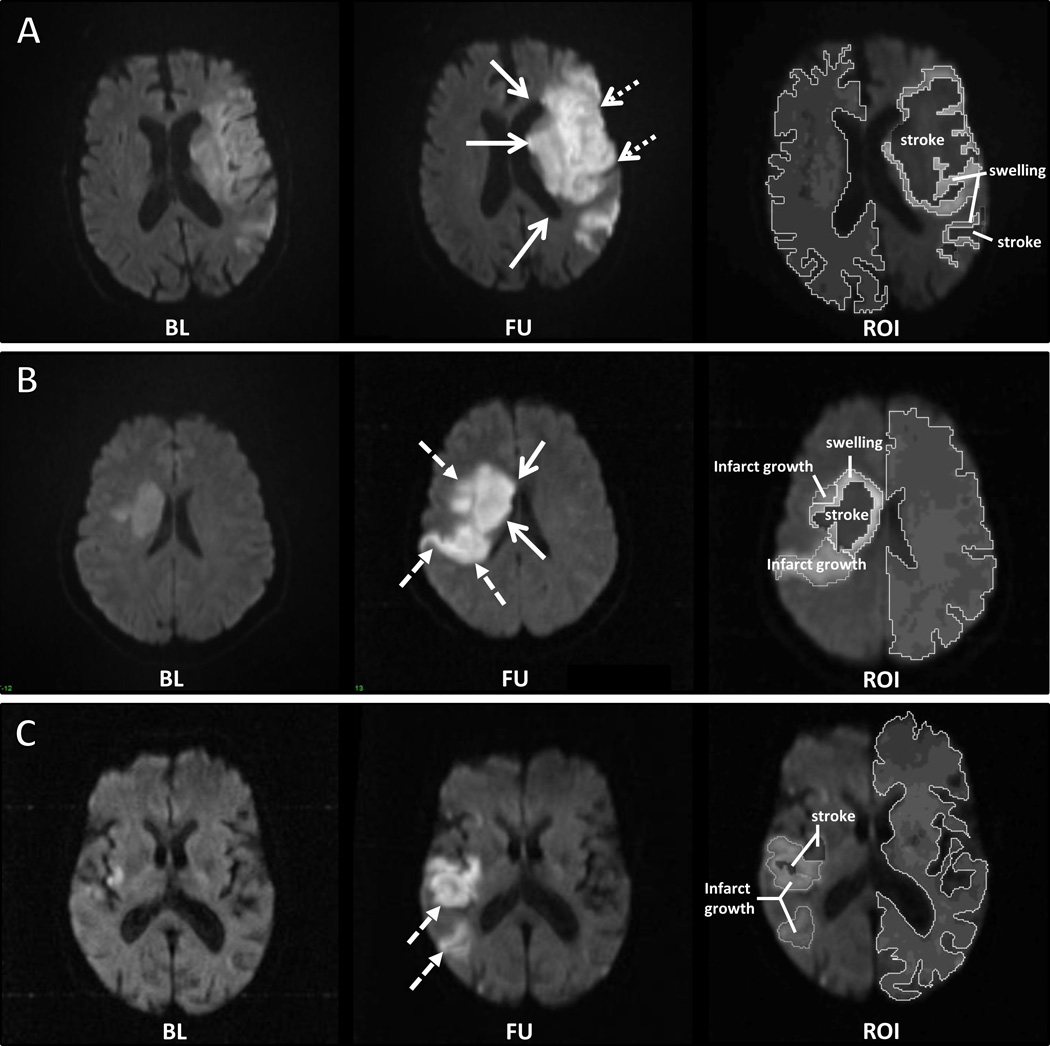
Methods: Two research cohorts of acute stroke subjects with serial brain MRI were analyzed. The categorical presence of swelling and infarct growth was assessed on diffusion-weighted imaging (DWI) by comparing baseline and follow-up scans. The increase in stroke volume (ΔDWI) was then subdivided into swelling and infarct growth volumes using region-of-interest analysis. The relationship of these imaging markers with outcome was evaluated in univariable and multivariable regression.
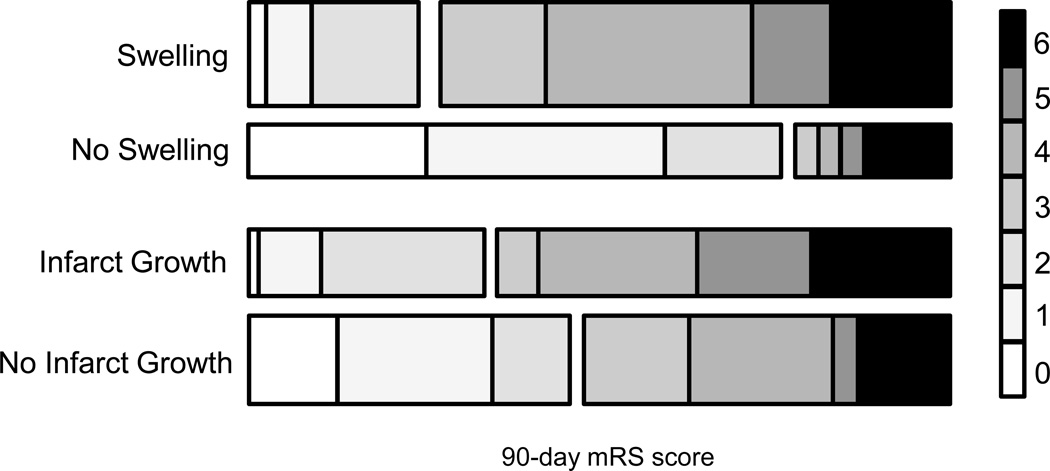
Results: The presence of swelling independently predicted worse outcome after adjustment for age, National Institutes of Health Stroke Scale, admission glucose, and baseline DWI volume (odds ratio, 4.55; 95% confidence interval, 1.21-18.9; P<0.02). Volumetric analysis confirmed that ΔDWI was associated with outcome (odds ratio, 4.29; 95% confidence interval, 2.00-11.5; P<0.001). After partitioning ΔDWI into swelling and infarct growth volumetrically, swelling remained an independent predictor of poor outcome (odds ratio, 1.09; 95% confidence interval, 1.03-1.17; P<0.005). Larger infarct growth was also associated with poor outcome (odds ratio, 7.05; 95% confidence interval, 1.04-143; P<0.045), although small infarct growth was not. The severity of cytotoxic injury measured on apparent diffusion coefficient maps was associated with swelling, whereas the perfusion deficit volume was associated with infarct growth.
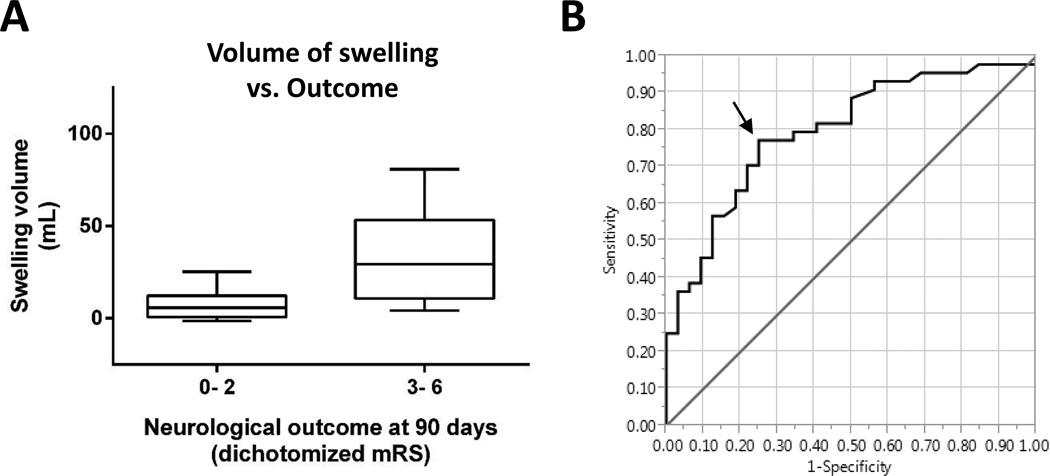
Conclusions: Swelling and infarct growth each contribute to total stroke lesion growth in the days after stroke. Swelling is an independent predictor of poor outcome, with a brain swelling volume of ≥11 mL identified as the threshold with greatest sensitivity and specificity for predicting poor outcome.
Keywords: brain edema; magnetic resonance imaging; stroke; swelling.
© 2014 American Heart Association, Inc.
Figures
References
-
- Wijdicks EF, Diringer MN. Middle cerebral artery territory infarction and early brain swelling: Progression and effect of age on outcome. Mayo Clinic proceedings. 1998;73:829–836. - PubMed
-
- Wijdicks EF, Sheth KN, Carter BS, Greer DM, Kasner SE, Kimberly WT, et al. Recommendations for the management of cerebral and cerebellar infarction with swelling: A statement for healthcare professionals from the american heart association/american stroke association. Stroke; a journal of cerebral circulation. 2014;45:1222–1238. - PubMed
-
- Hacke W, Schwab S, Horn M, Spranger M, De Georgia M, von Kummer R. 'Malignant' middle cerebral artery territory infarction: Clinical course and prognostic signs. Archives of neurology. 1996;53:309–315. - PubMed
-
- Berrouschot J, Sterker M, Bettin S, Koster J, Schneider D. Mortality of space-occupying ('malignant') middle cerebral artery infarction under conservative intensive care. Intensive care medicine. 1998;24:620–623. - PubMed
-
- Kimberly WT, Sheth KN. Approach to severe hemispheric stroke. Neurology. 2011;76:S50–S56. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
