

Pathological findings in cardiac apex removed during implantation of left ventricular assist devices (LVAD) are non-specific: 13-year-experience at a German Heart Center
- PMID: 25337196
- PMCID: PMC4203167
Pathological findings in cardiac apex removed during implantation of left ventricular assist devices (LVAD) are non-specific: 13-year-experience at a German Heart Center
Abstract
Background and aim: Ventricular assist devices (VAD) have become an established therapy for patients with end-stage heart failure. The two main reasons for this development are the shortage of appropriate donor organs and the increasing number of patients waiting for heart transplantation (HTX). Furthermore, the enormous advances in the technical equipment and the rising clinical experience have improved the implantation technique, the durability and the long-term patient outcomes.
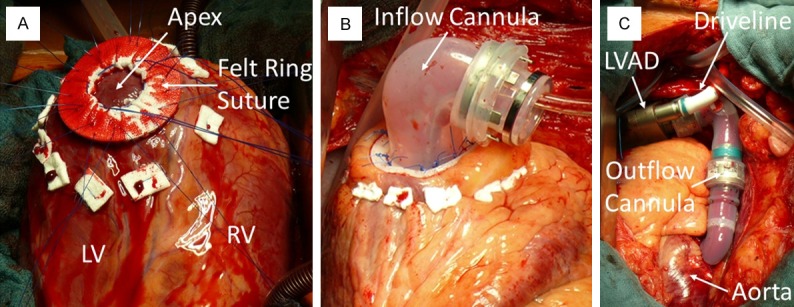
Methods: We reviewed all cases of left ventricular assist device (LVAD) implantation at our Erlangen Heart Center during January 2000-July 2013. The main aim of this study was to analyze the underlying pathology from the cardiac apex removed during the implantation. From all patients, we created a follow-up, analyzed the pathological features with the clinical diagnoses and described the overall outcome.
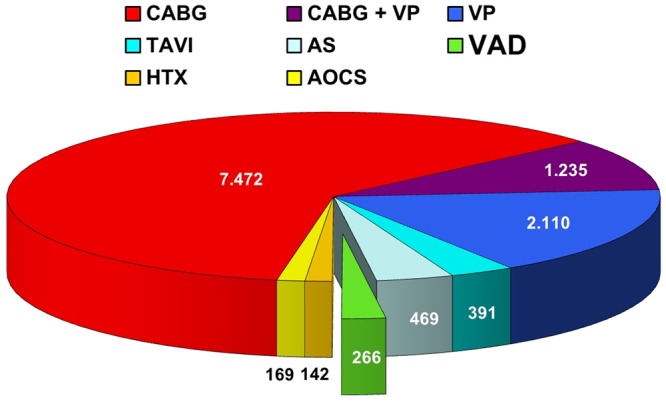
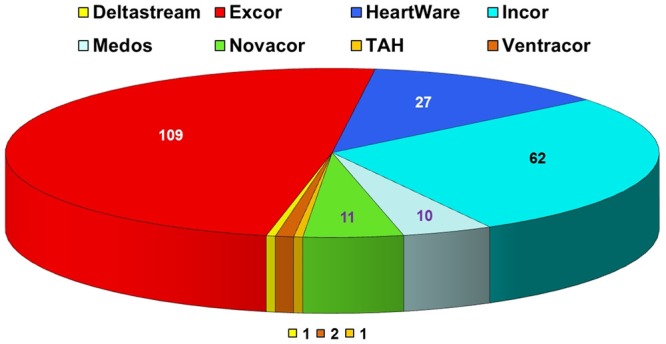
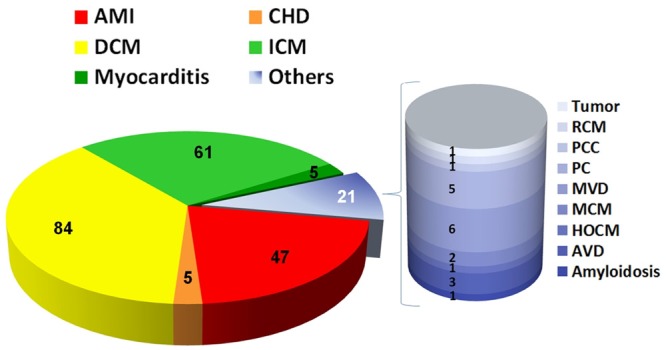
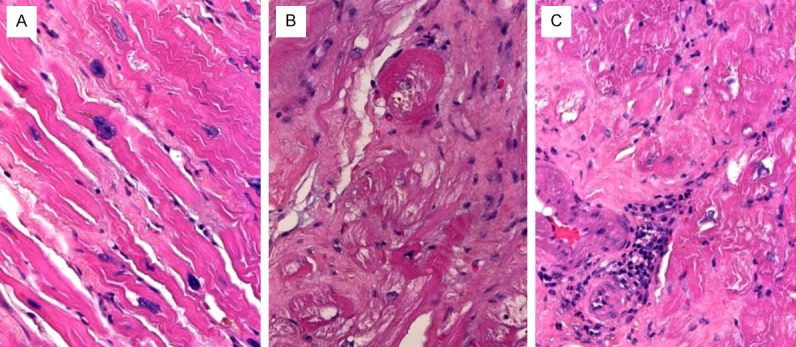
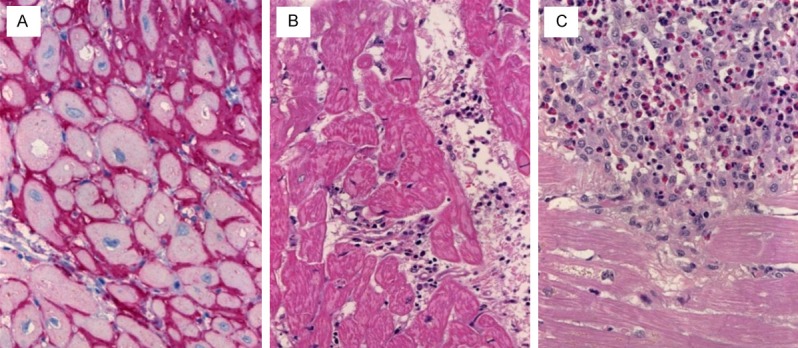
Results: VAD implantation was performed in 266 cases at our center in the last 13 years (2.2% of the total of 12254 cardiac surgical operations in that period). From these patients, 223 underwent LVAD or biventricular (BVAD) implantation; the remaining received a right (RVAD) implantation. The most frequent underlying clinical diagnoses were dilated (n = 84, 37.7%, DCM) or ischemic (n = 61, 27.4%, ICM) cardiomyopathy. The pathological findings in the apex biopsy were generally non-specific and showed variable interstitial myocardial fibrosis with evidence of fibre loss, fatty degeneration and variable irregular atrophy of muscle fibres, consistent with dilated and ischemic cardiomyopathies as the most frequent causes of heart failure in these patients. Only a few cases showed other specific features such as myocarditis and AL-amyloidosis.
Conclusions: Pathological findings in cardiac apex removed during LVAD implantation are rather non-specific and they generally reflect the late stage or consequences of chronic myocardial damage in cases of dilated or ischemic cardiomyopathies. Variable patchy chronic inflammatory changes may be observed in cardiomyopathies as a non-specific reaction caused by myocardial fiber damage and should not lead to misinterpretation as evidence of myocarditis or revision of original diagnosis.
Keywords: Left ventricular assist devices (LVAD); apex pathology; dilatative cardiomyopathy; ischemic cardiomyopathy; myocarditis.
Figures
References
-
- Moazami N, Hoercher KJ, Fukamachi K, Kobayashi M, Smedira NG, Massiello A, Horvath DJ. Mechanical circulatory support for heart failure: past, present and a look at the future. Expert Rev Med Devices. 2013;10:55–71. - PubMed
-
- Moosdorf R. Artificial heart and heart transplantation. Herz. 2012;37:869–74. - PubMed
-
- Carrel T, Englberger L, Martinelli MV, Takala J, Boesch C, Sigurdadottir V, Gygax E, Kadner A, Mohacsi P. Continuous flow left ventricular assist devices: a valid option for heart failure patients. Swiss Med Wkly. 2012;142:w13701. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous