

Primary gliosarcoma with long-survival: report of two cases and review of literature
- PMID: 25337286
- PMCID: PMC4203257
Primary gliosarcoma with long-survival: report of two cases and review of literature
Abstract
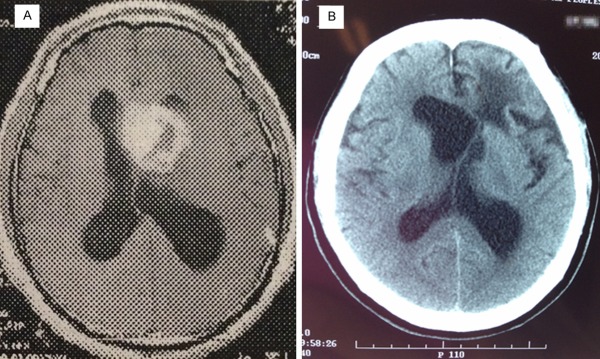
Background: Gliosarcoma (GS) is a rare high-grade malignant tumor with poor prognosis. The survival period of GS ranges from 4 to 18.5 months. Rarely would it be over 40 months. Survival of intraventricular GS is less than 8 months.
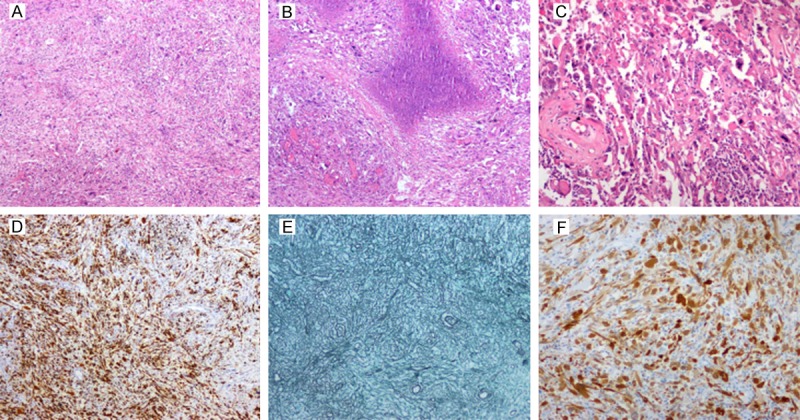
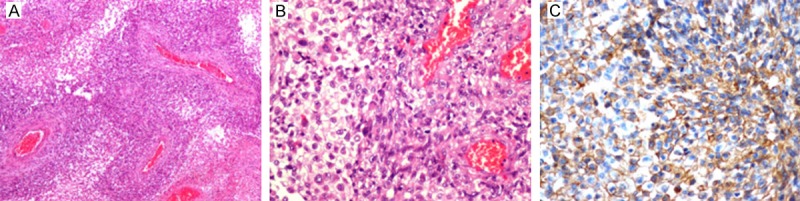
Methods: There were 2 cases of primary gliosarcoma in our hospital with long-term survival after resection, with one of pure intraventricular origin. We confirmed that our diagnosis was correct by light microscopy, GFAP immunohistochemistry and histochemistry of reticular fiber staining.
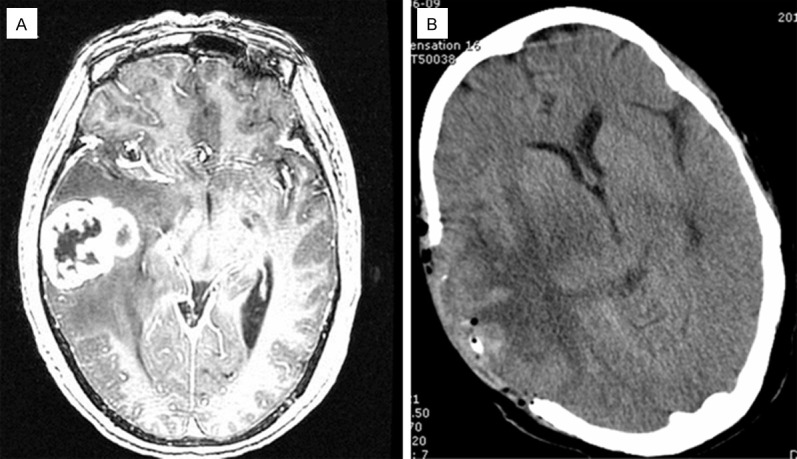
Results: In the first case, a 47-year-old man with intraventricular gliosarcoma survived for 130 months after surgery. In another case, a 63-year-old woman survived for 4 years after resection. Both cases of GS exhibited biphasic glioblastoma and fibrosarcoma with necrosis. According to the review of surgical records, complete tumor resections, including extended resections were carried out in both cases. The two patients received postoperative radiation therapy and chemotherapy without any further recurrence and metastasis.
Conclusions: We reported two cases of GS with long survival. The presented cases demonstrate that, in rare instances, gliosarcoma may show prolonged survival with after surgical excision combined with radiotherapy and chemotherapy.
Keywords: Primary gliosarcoma; intraventricular gliosarcoma; long survival.
Figures
References
-
- Louis DN, Ohgaki H, Wiestler OD, Cavenee WK. WHO classification of tumours of the central nervous system. 4th edition. Lyon: IARC; 2007. Gliosarcoma; pp. 48–49.
-
- Stroebe H. Ueber Entstehung und Bauder Gehirnglioma. Beitr Pathol Anat Allg Pathol. 1895;19:405–486.
-
- Feigin I, Allen LB, Lipkin L, Gross SW. The endothelial hyperplasia of the cerebral blood vessels with brain tumors, and its sarcomatous transformation. Cancer. 1958;11:264–277. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous