

Multiple advanced surgical techniques to treat acquired seminal duct obstruction
- PMID: 25337841
- PMCID: PMC4236339
- DOI: 10.4103/1008-682X.139256
Multiple advanced surgical techniques to treat acquired seminal duct obstruction
Abstract
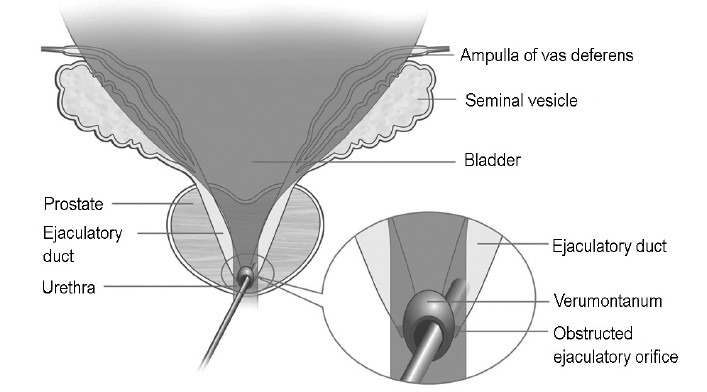
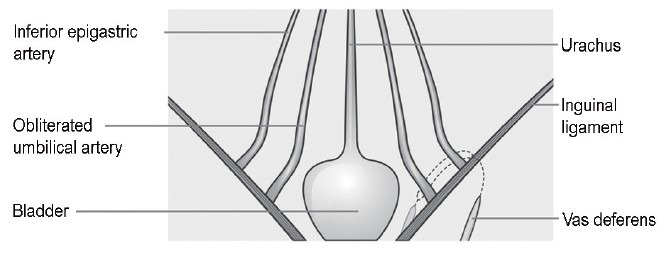
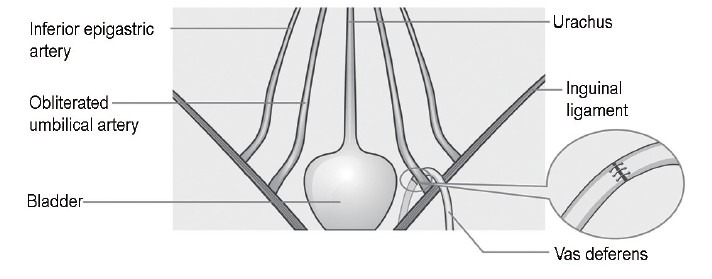
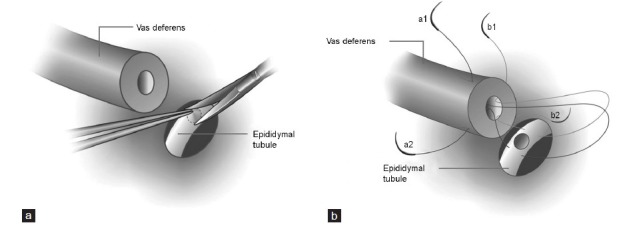
The aim of this study was to evaluate the outcomes of multiple advanced surgical treatments (i.e. microsurgery, laparoscopic surgery and endoscopic surgery) for acquired obstructive azoospermia. We analyzed the surgical outcomes of 51 patients with suspected acquired obstructive azoospermia consecutively who enrolled at our center between January 2009 and May 2013. Modified vasoepididymostomy, laparoscopically assisted vasovasostomy and transurethral incision of the ejaculatory duct with holmium laser were chosen and performed based on the different obstruction sites. The mean postoperative follow-up time was 22 months (range: 9 months to 52 months). Semen analyses were initiated at four postoperative weeks, followed by trimonthly (months 3, 6, 9 and 12) semen analyses, until no sperm was found at 12 months or until pregnancy was achieved. Patency was defined as >10,000 sperm ml⁻¹ of semen. The obstruction sites, postoperative patency and natural pregnancy rate were recorded. Of 51 patients, 47 underwent bilateral or unilateral surgical reconstruction; the other four patients were unable to be treated with surgical reconstruction because of pelvic vas or intratesticular tubules obstruction. The reconstruction rate was 92.2% (47/51), and the patency rate and natural pregnancy rate were 89.4% (42/47) and 38.1% (16/42), respectively. No severe complications were observed. Using multiple advanced surgical techniques, more extensive range of seminal duct obstruction was accessible and correctable; thus, a favorable patency and pregnancy rate can be achieved.
Figures
References
-
- Kolettis PN. Restructuring reconstructive techniques – advances in reconstructive techniques. Urol Clin North Am. 2008;35:229–34. viii. - PubMed
-
- Parekattil SJ, Gudeloglu A, Brahmbhatt J, Wharton J, Priola KB. Robotic assisted versus pure microsurgical vasectomy reversal: technique and prospective database control trial. J Reconstr Microsurg. 2012;28:435–44. - PubMed
-
- Shaeer OK, Shaeer KZ. Pelviscrotal vasovasostomy: refining and troubleshooting. J Urol. 2005;174:1935–7. - PubMed
-
- Goldstein M, Li PS, Matthews GJ. Microsurgical vasovasostomy: the microdot technique of precision suture placement. J Urol. 1998;159:188–90. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
