

Visual outcomes with flow-diverter stents covering the ophthalmic artery for treatment of internal carotid artery aneurysms
- PMID: 25339649
- PMCID: PMC7965674
- DOI: 10.3174/ajnr.A4129
Visual outcomes with flow-diverter stents covering the ophthalmic artery for treatment of internal carotid artery aneurysms
Abstract
Background and purpose: Flow-diverting stents can be used to treat intracranial aneurysms that are not amenable to treatment with coils. We analyzed ophthalmic consequences due to coverage of the origin of the ophthalmic artery by flow-diverting stents for the treatment of internal carotid artery aneurysms.
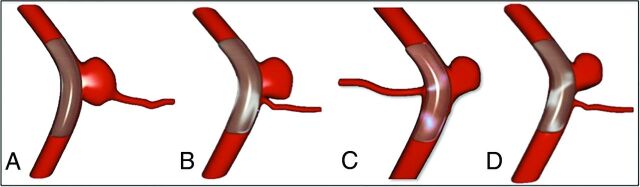
Materials and methods: From April 2009 to April 2013, the clinical and angiographic outcomes of all 28 patients treated for aneurysms with flow-diverting stents covering the origin of the ophthalmic artery were prospectively collected. The origin of the ophthalmic artery in relation to the target aneurysm was classified by using a 4-type classification. A complete ophthalmic examination was performed by a single ophthalmologist 48 hours before and 1 week after covering the ophthalmic artery.
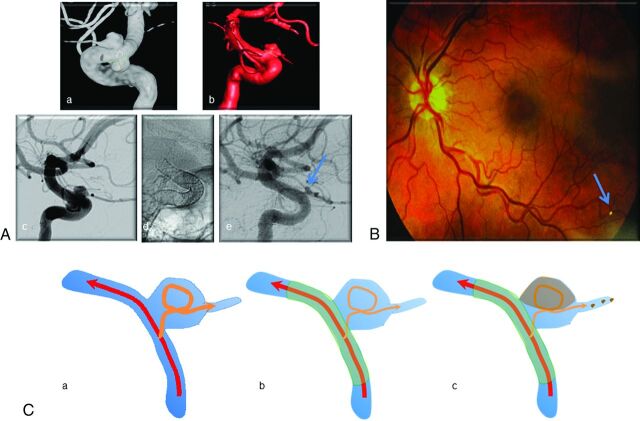
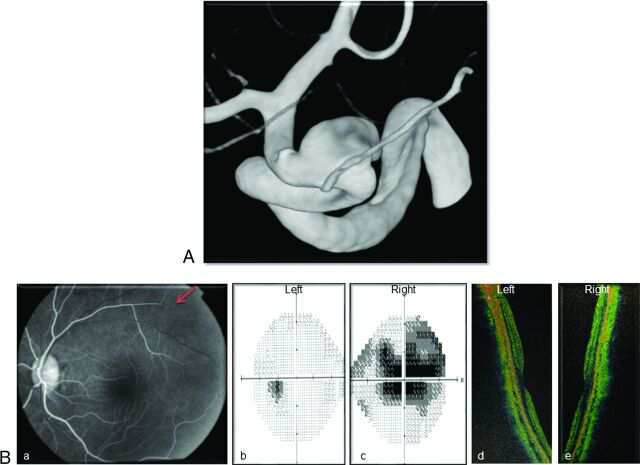
Results: Ophthalmic artery patency was normal at the end of endovascular treatment in 24/28 cases (85.7%). With extensive ophthalmic examinations, 11 patients (39.3%) showed new ophthalmic complications. Patients with the ophthalmic artery originating from the aneurysm sac were at high risk for retinal emboli (4/5, 80%). Patients with the ophthalmic artery originating from the inner curve of the carotid siphon were at high risk for optic nerve ischemic atrophy (3/4, 75%).
Conclusions: This prospective study shows that covering the ophthalmic artery with a flow-diverting stent is not without potential complications. Ophthalmic complications can occur but are often not diagnosed. The anatomic disposition of the ophthalmic artery in relation to the carotid siphon and aneurysm should be clearly understood because some configurations have a higher risk. When not required, covering of the ophthalmic artery by flow-diverting stents should be avoided.
© 2015 by American Journal of Neuroradiology.
Figures
References
-
- Brinjikji W, Murad MH, Lanzino G, et al. . Endovascular treatment of intracranial aneurysms with flow diverters: a meta-analysis. Stroke 2013;44:442–47 - PubMed
-
- Fiorella D, Woo HH, Albuquerque FC, et al. . Definitive reconstruction of circumferential, fusiform intracranial aneurysms with the Pipeline embolization device. Neurosurgery 2008;62:1115–20; discussion 1120–21 - PubMed
-
- Pistocchi S, Blanc R, Bartolini B, et al. . Flow diverters at and beyond the level of the circle of Willis for the treatment of intracranial aneurysms. Stroke 2012;43:1032–38 - PubMed
-
- Lylyk P, Miranda C, Ceratto R, et al. . Curative endovascular reconstruction of cerebral aneurysms with the Pipeline embolization device: the Buenos Aires experience. Neurosurgery 2009;64:632–42; discussion 642–43 - PubMed
-
- D'Urso PI, Lanzino G, Cloft HJ, et al. . Flow diversion for intracranial aneurysms: a review. Stroke 2011;42:2363–68 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous