

Robotic surgery for rectal cancer: current immediate clinical and oncological outcomes
- PMID: 25339823
- PMCID: PMC4202365
- DOI: 10.3748/wjg.v20.i39.14359
Robotic surgery for rectal cancer: current immediate clinical and oncological outcomes
Abstract
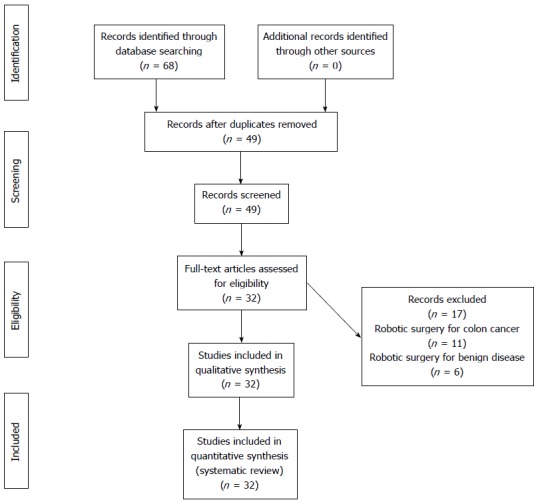
Laparoscopic rectal surgery continues to be a challenging operation associated to a steep learning curve. Robotic surgical systems have dramatically changed minimally invasive surgery. Three-dimensional, magnified and stable view, articulated instruments, and reduction of physiologic tremors leading to superior dexterity and ergonomics. Therefore, robotic platforms could potentially address limitations of laparoscopic rectal surgery. It was aimed at reviewing current literature on short-term clinical and oncological (pathological) outcomes after robotic rectal cancer surgery in comparison with laparoscopic surgery. A systematic review was performed for the period 2002 to 2014. A total of 1776 patients with rectal cancer underwent minimally invasive robotic treatment in 32 studies. After robotic and laparoscopic approach to oncologic rectal surgery, respectively, mean operating time varied from 192-385 min, and from 158-297 min; mean estimated blood loss was between 33 and 283 mL, and between 127 and 300 mL; mean length of stay varied from 4-10 d; and from 6-15 d. Conversion after robotic rectal surgery varied from 0% to 9.4%, and from 0 to 22% after laparoscopy. There was no difference between robotic (0%-41.3%) and laparoscopic (5.5%-29.3%) surgery regarding morbidity and anastomotic complications (respectively, 0%-13.5%, and 0%-11.1%). Regarding immediate oncologic outcomes, respectively among robotic and laparoscopic cases, positive circumferential margins varied from 0% to 7.5%, and from 0% to 8.8%; the mean number of retrieved lymph nodes was between 10 and 20, and between 11 and 21; and the mean distal resection margin was from 0.8 to 4.7 cm, and from 1.9 to 4.5 cm. Robotic rectal cancer surgery is being undertaken by experienced surgeons. However, the quality of the assembled evidence does not support definite conclusions about most studies variables. Robotic rectal cancer surgery is associated to increased costs and operating time. It also seems to be associated to reduced conversion rates. Other short-term outcomes are comparable to conventional laparoscopy techniques, if not better. Ultimately, pathological data evaluation suggests that oncologic safety may be preserved after robotic total mesorectal excision. However, further studies are required to evaluate oncologic safety and functional results.
Keywords: Colorectal surgery; Minimally invasive; Rectal neoplasms; Robotics; Surgical procedures.
Figures
References
-
- Jacobs M, Verdeja JC, Goldstein HS. Minimally invasive colon resection (laparoscopic colectomy) Surg Laparosc Endosc. 1991;1:144–150. - PubMed
-
- Clinical Outcomes of Surgical Therapy Study Group. A comparison of laparoscopically assisted and open colectomy for colon cancer. N Engl J Med. 2004;350:2050–2059. - PubMed
-
- Gaertner WB, Kwaan MR, Madoff RD, Willis D, Belzer GE, Rothenberger DA, Melton GB. The evolving role of laparoscopy in colonic diverticular disease: a systematic review. World J Surg. 2013;37:629–638. - PubMed
-
- Siddiqui MR, Sajid MS, Khatri K, Cheek E, Baig MK. Elective open versus laparoscopic sigmoid colectomy for diverticular disease: a meta-analysis with the Sigma trial. World J Surg. 2010;34:2883–2901. - PubMed
-
- Di B, Li Y, Wei K, Xiao X, Shi J, Zhang Y, Yang X, Gao P, Zhang K, Yuan Y, et al. Laparoscopic versus open surgery for colon cancer: a meta-analysis of 5-year follow-up outcomes. Surg Oncol. 2013;22:e39–e43. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
