

Migraine and stroke: "vascular" comorbidity
- PMID: 25339937
- PMCID: PMC4189436
- DOI: 10.3389/fneur.2014.00193
Migraine and stroke: "vascular" comorbidity
Abstract
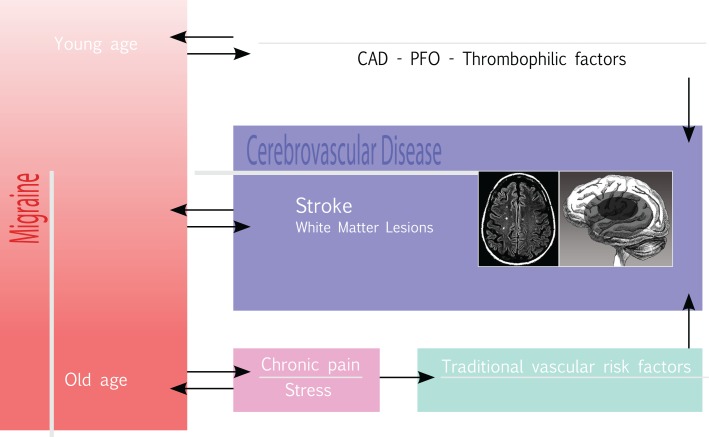
Several comorbidities are associated to migraine. Recent meta-analyses have consistently demonstrated a relationship between migraine and stroke, which is well-defined for ischemic stroke and migraine with aura (MA), even stronger in females on oral contraceptives or smokers. However, there seems to be no clear-cut association between stroke in migraineurs and the common vascular risk factors, at least in the young adult population. Migraineurs also run an increased risk of hemorrhagic stroke, while the association between migraine and cardiovascular disease remains poorly defined. Another aspect is the relationship between migraine and the presence of silent brain lesions. It has been demonstrated that there is an increased frequency of ischemic lesions in the white matter of migraineurs, especially silent infarcts in the posterior circulation territory in patients with at least 10 attacks per month. Although there is a higher prevalence of patent foramen ovale (PFO) in migraineurs, the relationship between migraine and PFO remains controversial and PFO closure is not a recommended procedure to prevent migraine. As an increased frequency of cervical artery dissections has been observed in migrainous patients, it has been hypothesized that migraine may represent a predisposing factor for cervical artery dissection. There still remains the question as to whether migraine should be considered a true "vascular disease" or if the comorbidity between migraine and cerebrovascular disease may have underlying shared risk factors or pathophysiological mechanisms. Although further studies are required to clarify this issue, current evidence supports a clinical management where MA patients should be screened for other concomitant vascular risk factors and treated accordingly.
Keywords: cerebrovascular disease; hemorrhagic stroke; ischemic stroke; migraine; stroke; vascular risk factors.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous