

Antibodies to MOG have a demyelination phenotype and affect oligodendrocyte cytoskeleton
- PMID: 25340056
- PMCID: PMC4202678
- DOI: 10.1212/NXI.0000000000000012
Antibodies to MOG have a demyelination phenotype and affect oligodendrocyte cytoskeleton
Abstract
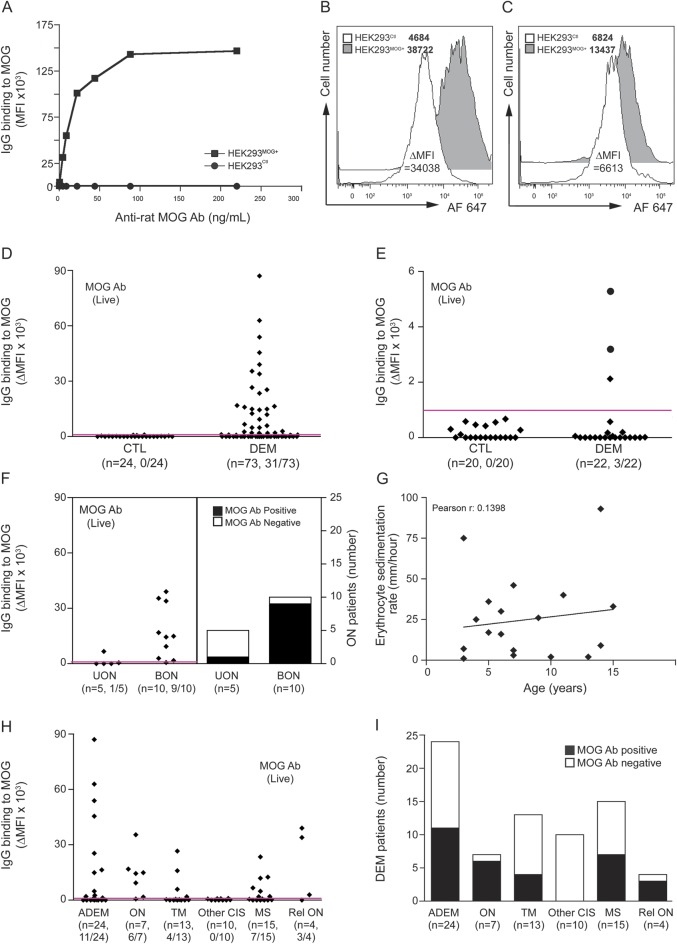
Objective: To examine the clinical features of pediatric CNS demyelination associated with positive myelin oligodendrocyte glycoprotein (MOG) antibodies and to examine the functional effects of MOG antibody on oligodendrocyte cytoskeleton.
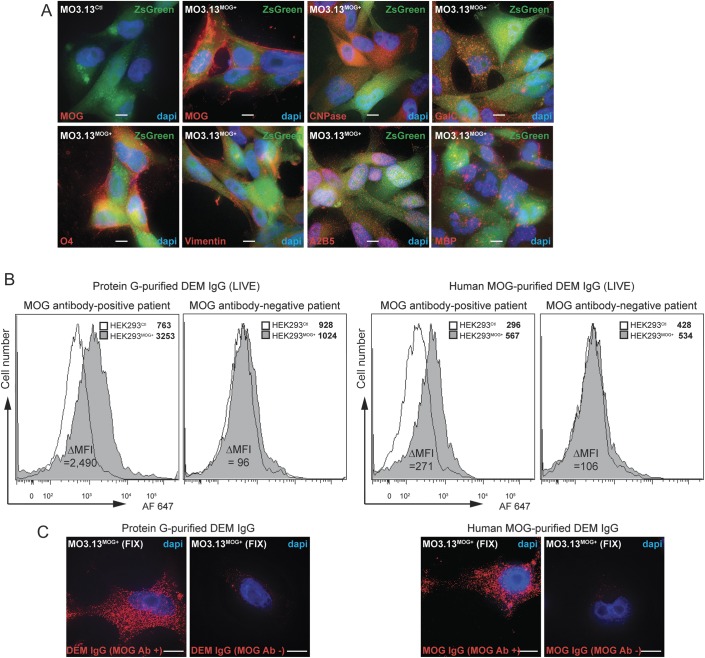
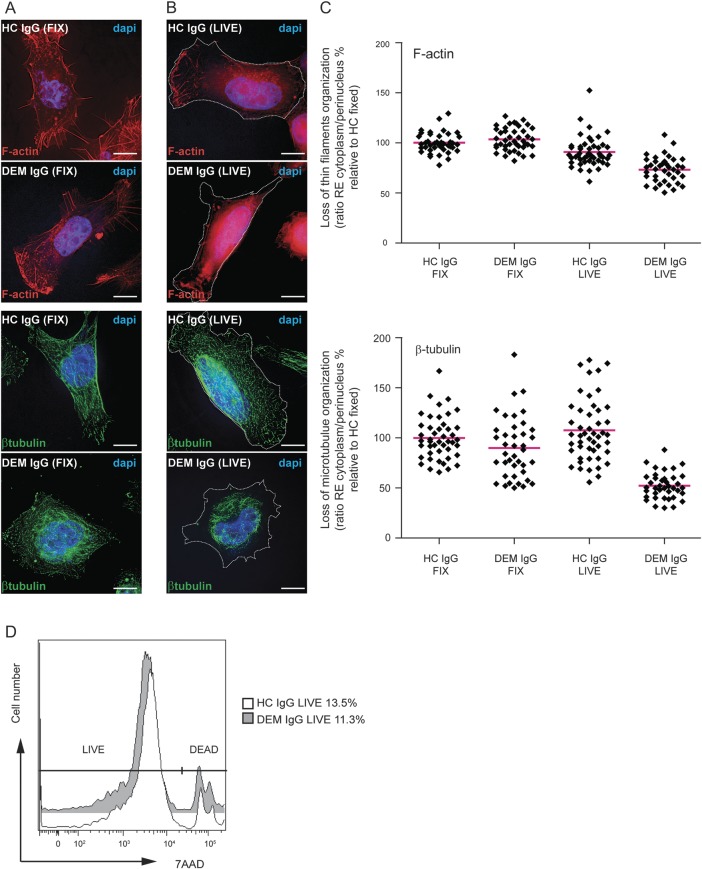
Methods: We measured MOG antibody using a fluorescence-activated cell sorting live cell-based assay in acute sera of 73 children with CNS demyelination (DEM) (median age 8 years, range 1.3-15.3) followed for a median of 4 years. We used MO3.13 cells to examine immunoglobulin (Ig) G effects on oligodendrocyte cytoskeleton using 3D deconvolution imaging.
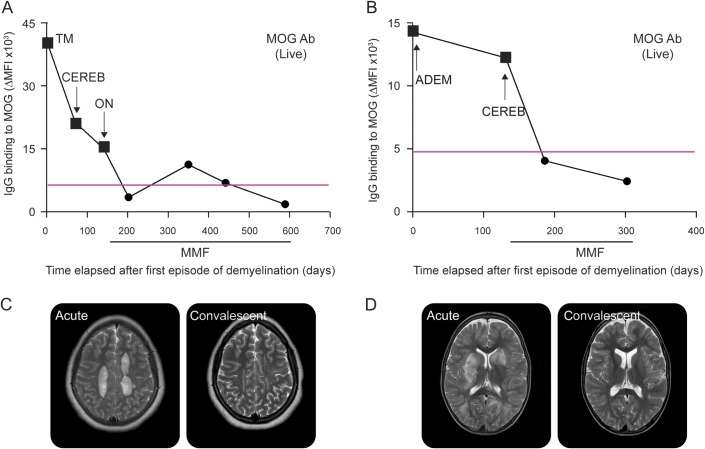
Results: MOG antibodies were found in 31/73 patients with DEM (42%) but in 0/24 controls. At first presentation, MOG antibody-positive patients were more likely to have bilateral than unilateral optic neuritis (ON) (9/10 vs 1/5, respectively, p = 0.03), less likely to have brainstem findings (2/31 vs 16/42, p = 0.005), more likely to have a raised erythrocyte sedimentation rate >20 mm/h (9/19 vs 3/21, p = 0.05), less likely to have intrathecal oligoclonal bands (0/16 vs 5/27, p = 0.18), and less likely to be homozygous or heterozygous for human leukocyte antigen DRB1*1501 (3/18 vs 7/22, p = 0.46). MOG antibody positivity varied according to clinical phenotype, with ON and relapsing ON most likely to be seropositive. Two relapsing MOG antibody-positive patients treated with mycophenolate mofetil remain in remission and have become MOG antibody seronegative. Oligodendrocytes incubated with purified IgG from MOG antibody-positive patients showed a striking loss of organization of the thin filaments and the microtubule cytoskeleton, as evidenced by F-actin and β-tubulin immunolabelings.
Conclusions: MOG antibody may define a separate demyelination syndrome, which has therapeutic implications. MOG antibody has functional effects on oligodendrocyte cytoskeleton.
Figures
References
-
- Vincent A, Bien CG, Irani SR, Waters P. Autoantibodies associated with diseases of the CNS: new developments and future challenges. Lancet Neurol 2011;10:759–772 - PubMed
-
- Wingerchuk DM, Lennon VA, Lucchinetti CF, Pittock SJ, Weinshenker BG. The spectrum of neuromyelitis optica. Lancet Neurol 2007;6:805–815 - PubMed
-
- Johns TG, Bernard CC. The structure and function of myelin oligodendrocyte glycoprotein. J Neurochem 1999;72:1–9 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous