

Multi-scale symbolic entropy analysis provides prognostic prediction in patients receiving extracorporeal life support
- PMID: 25341381
- PMCID: PMC4221713
- DOI: 10.1186/s13054-014-0548-3
Multi-scale symbolic entropy analysis provides prognostic prediction in patients receiving extracorporeal life support
Abstract
Introduction: Extracorporeal life support (ECLS) can temporarily support cardiopulmonary function, and is occasionally used in resuscitation. Multi-scale entropy (MSE) derived from heart rate variability (HRV) is a powerful tool in outcome prediction of patients with cardiovascular diseases. Multi-scale symbolic entropy analysis (MSsE), a new method derived from MSE, mitigates the effect of arrhythmia on analysis. The objective is to evaluate the prognostic value of MSsE in patients receiving ECLS. The primary outcome is death or urgent transplantation during the index admission.
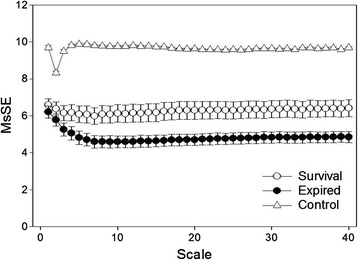
Methods: Fifty-seven patients receiving ECLS less than 24 hours and 23 control subjects were enrolled. Digital 24-hour Holter electrocardiograms were recorded and three MSsE parameters (slope 5, Area 6-20, Area 6-40) associated with the multiscale correlation and complexity of heart beat fluctuation were calculated.
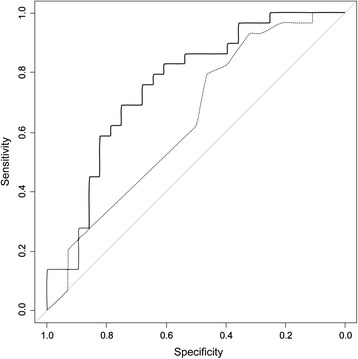
Results: Patients receiving ECLS had significantly lower value of slope 5, area 6 to 20, and area 6 to 40 than control subjects. During the follow-up period, 29 patients met primary outcome. Age, slope 5, Area 6 to 20, Area 6 to 40, acute physiology and chronic health evaluation II score, multiple organ dysfunction score (MODS), logistic organ dysfunction score (LODS), and myocardial infarction history were significantly associated with primary outcome. Slope 5 showed the greatest discriminatory power. In a net reclassification improvement model, slope 5 significantly improved the predictive power of LODS; Area 6 to 20 and Area 6 to 40 significantly improved the predictive power in MODS. In an integrated discrimination improvement model, slope 5 added significantly to the prediction power of each clinical parameter. Area 6 to 20 and Area 6 to 40 significantly improved the predictive power in sequential organ failure assessment.
Conclusions: MSsE provides additional prognostic information in patients receiving ECLS.
Figures


References
-
- Chen YS, Lin JW, Yu HY, Ko WJ, Jerng JS, Chang WT, Chen WJ, Huang SC, Chi NH, Wang CH, Chen LC, Tsai PR, Wang SS, Hwang JJ, Lin FY. Cardiopulmonary resuscitation with assisted extracorporeal life-support versus conventional cardiopulmonary resuscitation in adults with in-hospital cardiac arrest: an observational study and propensity analysis. Lancet. 2008;372:554–561. doi: 10.1016/S0140-6736(08)60958-7. - DOI - PubMed
-
- Pappalardo F, Pieri M, Greco T, Patroniti N, Pesenti A, Arcadipane A, Ranieri VM, Gattinoni L, Landoni G, Holzgraefe B, Beutel G, Zangrillo A, Italian ECMOnet Predicting mortality risk in patients undergoing venovenous ECMO for ARDS due to influenza A (H1N1) pneumonia: the ECMOnet score. Intensive Care Med. 2013;39:275–281. doi: 10.1007/s00134-012-2747-1. - DOI - PMC - PubMed
-
- Hsu KH, Chi NH, Yu HY, Wang CH, Huang SC, Wang SS, Ko WJ, Chen YS. Extracorporeal membranous oxygenation support for acute fulminant myocarditis: analysis of a single center’s experience. Eur J Cardiothorac Surg. 2011;40:682–688. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
