

Defining the complement biomarker profile of C3 glomerulopathy
- PMID: 25341722
- PMCID: PMC4220750
- DOI: 10.2215/CJN.01820214
Defining the complement biomarker profile of C3 glomerulopathy
Abstract
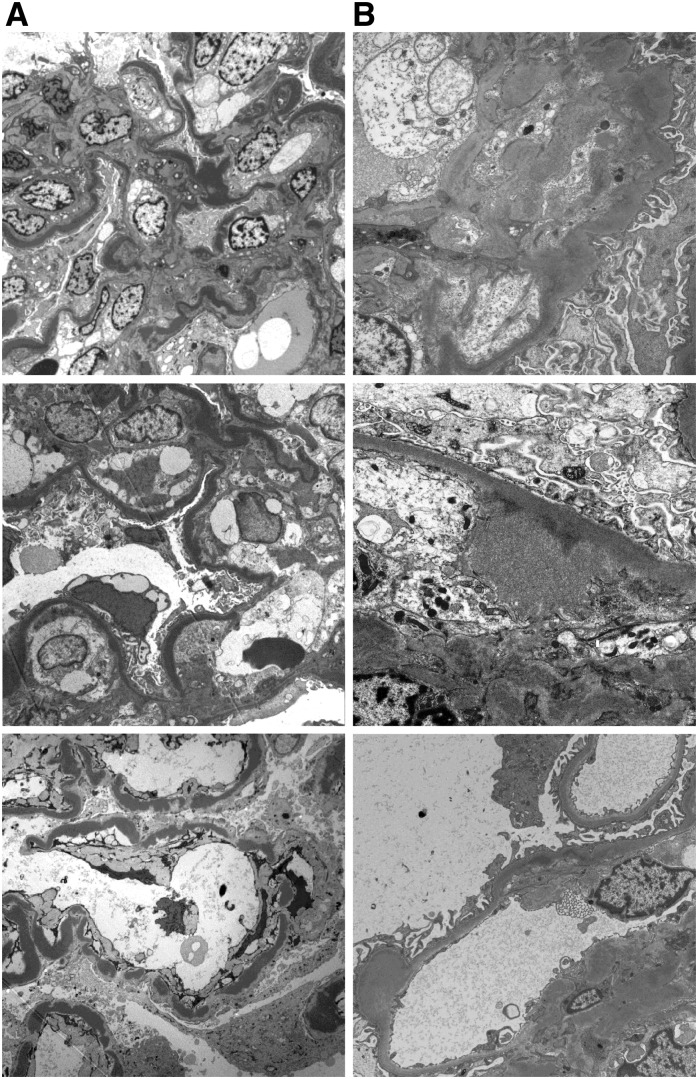
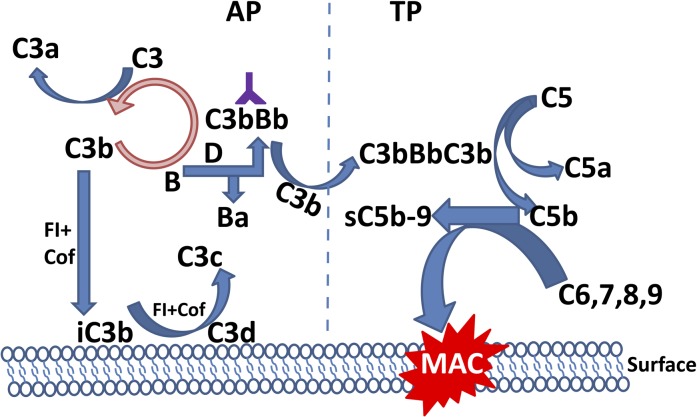
Background and objectives: C3 glomerulopathy (C3G) applies to a group of renal diseases defined by a specific renal biopsy finding: a dominant pattern of C3 fragment deposition on immunofluorescence. The primary pathogenic mechanism involves abnormal control of the alternative complement pathway, although a full description of the disease spectrum remains to be determined. This study sought to validate and define the association of complement dysregulation with C3G and to determine whether specific complement pathway abnormalities could inform disease definition.
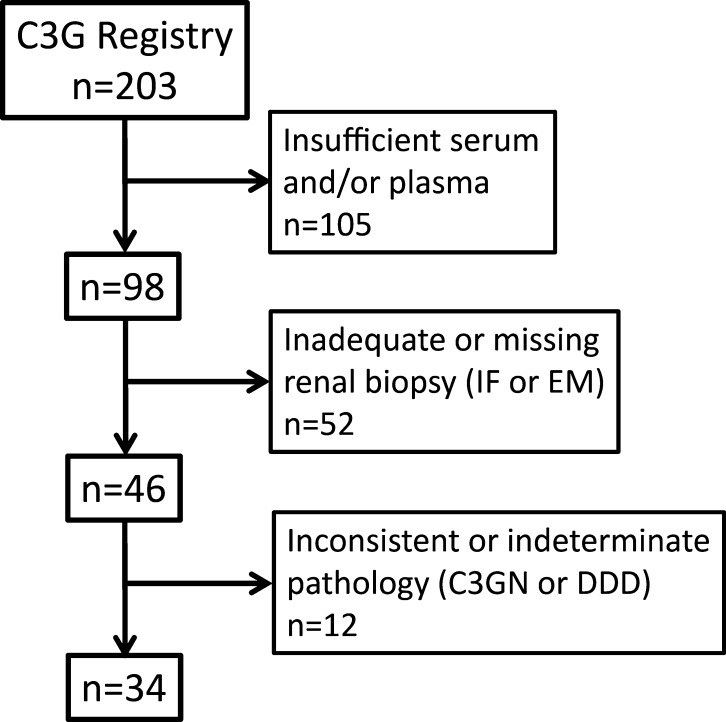
Design, setting, participants, & measurements: This study included 34 patients with C3G (17 with C3 glomerulonephritis [C3GN] and 17 with dense deposit disease [DDD]) diagnosed between 2008 and 2013 selected from the C3G Registry. Control samples (n=100) were recruited from regional blood drives. Nineteen complement biomarkers were assayed on all samples. Results were compared between C3G disease categories and with normal controls.
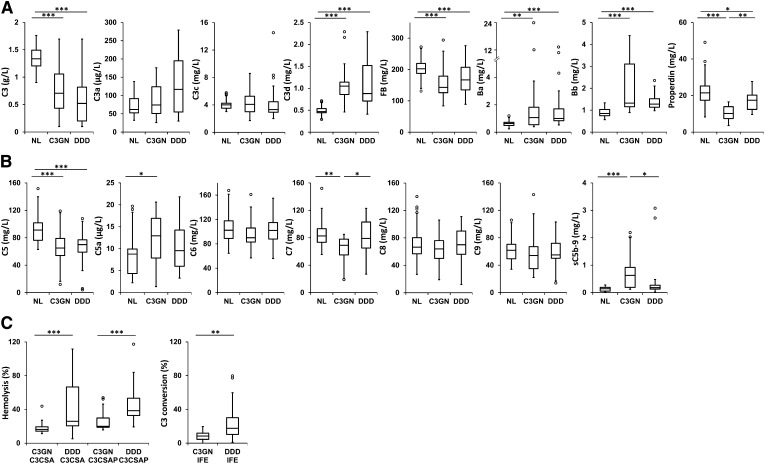
Results: Assessment of the alternative complement pathway showed that compared with controls, patients with C3G had lower levels of serum C3 (P<0.001 for both DDD and C3GN) and factor B (P<0.001 for both DDD and C3GN) as well as higher levels of complement breakdown products including C3d (P<0.001 for both DDD and C3GN) and Bb (P<0.001 for both DDD and C3GN). A comparison of terminal complement pathway proteins showed that although C5 levels were significantly suppressed (P<0.001 for both DDD and C3GN) its breakdown product C5a was significantly higher only in patients with C3GN (P<0.05). Of the other terminal pathway components (C6-C9), the only significant difference was in C7 levels between patients with C3GN and controls (P<0.01). Soluble C5b-9 was elevated in both diseases but only the difference between patients with C3GN and controls reached statistical significance (P<0.001). Levels of C3 nephritic factor activity were qualitatively higher in patients with DDD compared with patients with C3GN.
Conclusions: Complement biomarkers are significantly abnormal in patients with C3G compared with controls. These data substantiate the link between complement dysregulation and C3G and identify C3G interdisease differences.
Keywords: C3 glomerulopathy; C3GN; alternative pathway; complement; dense deposit disease.
Copyright © 2014 by the American Society of Nephrology.
Figures
Comment in
-
Circulating complement levels and C3 glomerulopathy.Clin J Am Soc Nephrol. 2014 Nov 7;9(11):1829-31. doi: 10.2215/CJN.09620914. Epub 2014 Oct 23. Clin J Am Soc Nephrol. 2014. PMID: 25341723 Free PMC article. No abstract available.
References
-
- Nester CM, Smith RJ: Diagnosis and treatment of C3 glomerulopathy. Clin Nephrol 80: 395–403, 2013 - PubMed
-
- Servais A, Noël LH, Frémeaux-Bacchi V, Lesavre P: C3 glomerulopathy. Contrib Nephrol 181: 185–193, 2013 - PubMed
-
- Pickering MC, D’Agati VD, Nester CM, Smith RJ, Haas M, Appel GB, Alpers CE, Bajema IM, Bedrosian C, Braun M, Doyle M, Fakhouri F, Fervenza FC, Fogo AB, Frémeaux-Bacchi V, Gale DP, Goicoechea de Jorge E, Griffin G, Harris CL, Holers VM, Johnson S, Lavin PJ, Medjeral-Thomas N, Paul Morgan B, Nast CC, Noel LH, Peters DK, Rodríguez de Córdoba S, Servais A, Sethi S, Song WC, Tamburini P, Thurman JM, Zavros M, Cook HT: C3 glomerulopathy: Consensus report. Kidney Int 84: 1079–1089, 2013 - PMC - PubMed
-
- Walker PD, Ferrario F, Joh K, Bonsib SM: Dense deposit disease is not a membranoproliferative glomerulonephritis. Mod Pathol 20: 605–616, 2007 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
