

Risk of fracture in urolithiasis: a population-based cohort study using the health improvement network
- PMID: 25341724
- PMCID: PMC4255404
- DOI: 10.2215/CJN.04340514
Risk of fracture in urolithiasis: a population-based cohort study using the health improvement network
Abstract
Background and objectives: Studies have shown decreased bone mineral density in individuals with urolithiasis, but their burden of fracture remains unclear. This study sought to determine whether urolithiasis is associated with increased fracture risk across the lifespan and to delineate sex effects.
Design, setting, participants, & measurements: A population-based retrospective cohort study using The Health Improvement Network was performed. The median calendar year for the start of the observation period was 2004 (1994-2012). This study identified 51,785 participants with ≥1 of 87 diagnostic codes for urolithiasis and 517,267 randomly selected age-, sex-, and practice-matched participants. Cox regression was used to estimate the hazard ratio (HR) for first fracture. Fractures identified using diagnostic codes were classified by anatomic site.
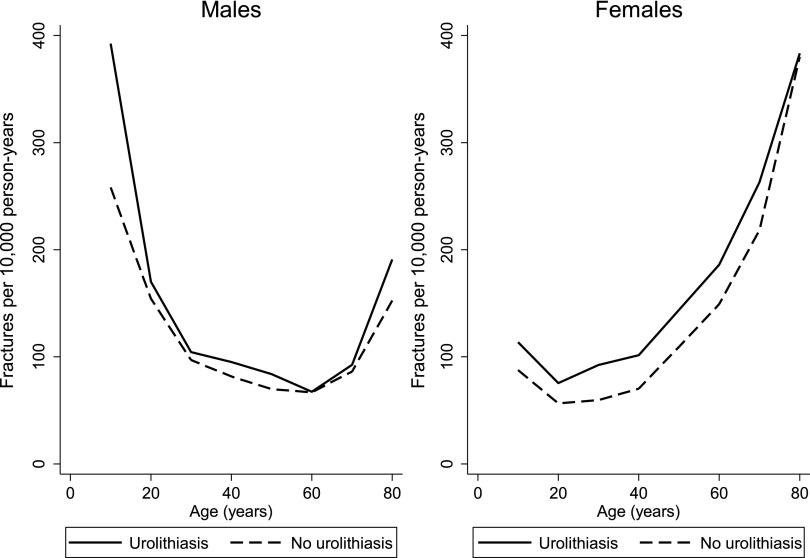
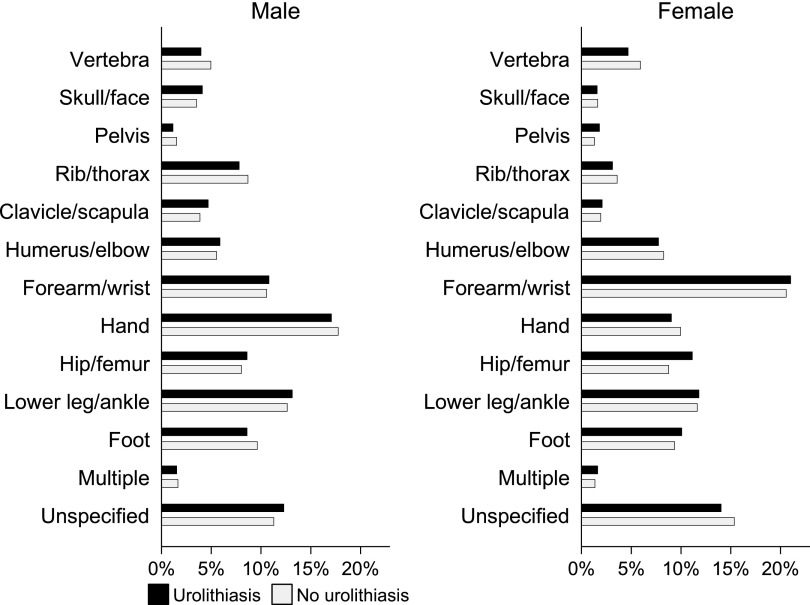
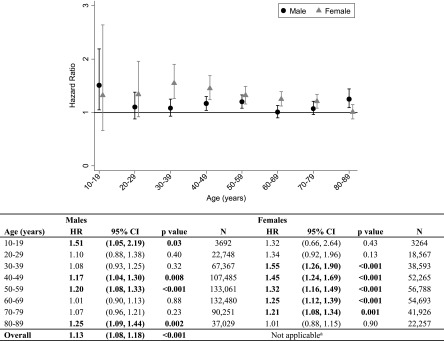
Results: Median age was 53 years, and 67% of participants were men, confirming their greater urolithiasis burden. Median time from urolithiasis diagnosis to fracture was 10 years. The HR for fracture associated with urolithiasis differed by sex and age (P for interactions, P≤0.003). In men, the adjusted HR was greatest in adolescence (1.55; 95% confidence interval [95% CI], 1.07 to 2.25) with an overall HR of 1.10 (95% CI, 1.05 to 1.16). Urolithiasis was associated with higher fracture risk in women aged 30-79 years (HR, 1.17-1.52), and was highest in women aged 30-39 years (HR, 1.52; 95% CI, 1.23 to 1.87). Peak background fracture rates were highest in boys aged 10-19 years and in women aged 70-79 years. The incidence per 10,000 person-years in participants with versus without urolithiasis was 392 versus 258 in male participants aged 10-19 years, and 263 versus 218 in women aged 70-79 years. Distribution of fracture site within sex did not differ between participants with versus without urolithiasis.
Conclusions: Urolithiasis was associated with higher incident fracture risk. The significantly higher risk at times of peak background fracture incidence in adolescent boys and elderly women has profound public health implications.
Keywords: epidemiology and outcomes; kidney stones; risk factors.
Copyright © 2014 by the American Society of Nephrology.
Figures
Comment in
-
Stones: Bone health in patients with kidney stones.Nat Rev Urol. 2015 Jan;12(1):9-10. doi: 10.1038/nrurol.2014.333. Epub 2014 Dec 9. Nat Rev Urol. 2015. PMID: 25487049 No abstract available.
References
-
- Stamatelou KK, Francis ME, Jones CA, Nyberg LM, Curhan GC: Time trends in reported prevalence of kidney stones in the United States: 1976-1994. Kidney Int 63: 1817–1823, 2003 - PubMed
-
- Eisner BH, Porten SP, Bechis SK, Stoller ML: Diabetic kidney stone formers excrete more oxalate and have lower urine pH than nondiabetic stone formers. J Urol 183: 2244–2248, 2010 - PubMed
-
- Taylor EN, Stampfer MJ, Curhan GC: Obesity, weight gain, and the risk of kidney stones. JAMA 293: 455–462, 2005 - PubMed
-
- Coe FL, Keck J, Norton ER: The natural history of calcium urolithiasis. JAMA 238: 1519–1523, 1977 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
