

Feasibility of AmbulanCe-Based Telemedicine (FACT) study: safety, feasibility and reliability of third generation in-ambulance telemedicine
- PMID: 25343246
- PMCID: PMC4208882
- DOI: 10.1371/journal.pone.0110043
Feasibility of AmbulanCe-Based Telemedicine (FACT) study: safety, feasibility and reliability of third generation in-ambulance telemedicine
Abstract
Background: Telemedicine is currently mainly applied as an in-hospital service, but this technology also holds potential to improve emergency care in the prehospital arena. We report on the safety, feasibility and reliability of in-ambulance teleconsultation using a telemedicine system of the third generation.
Methods: A routine ambulance was equipped with a system for real-time bidirectional audio-video communication, automated transmission of vital parameters, glycemia and electronic patient identification. All patients ( ≥ 18 years) transported during emergency missions by a Prehospital Intervention Team of the Universitair Ziekenhuis Brussel were eligible for inclusion. To guarantee mobility and to facilitate 24/7 availability, the teleconsultants used lightweight laptop computers to access a dedicated telemedicine platform, which also provided functionalities for neurological assessment, electronic reporting and prehospital notification of the in-hospital team. Key registrations included any safety issue, mobile connectivity, communication of patient information, audiovisual quality, user-friendliness and accuracy of the prehospital diagnosis.
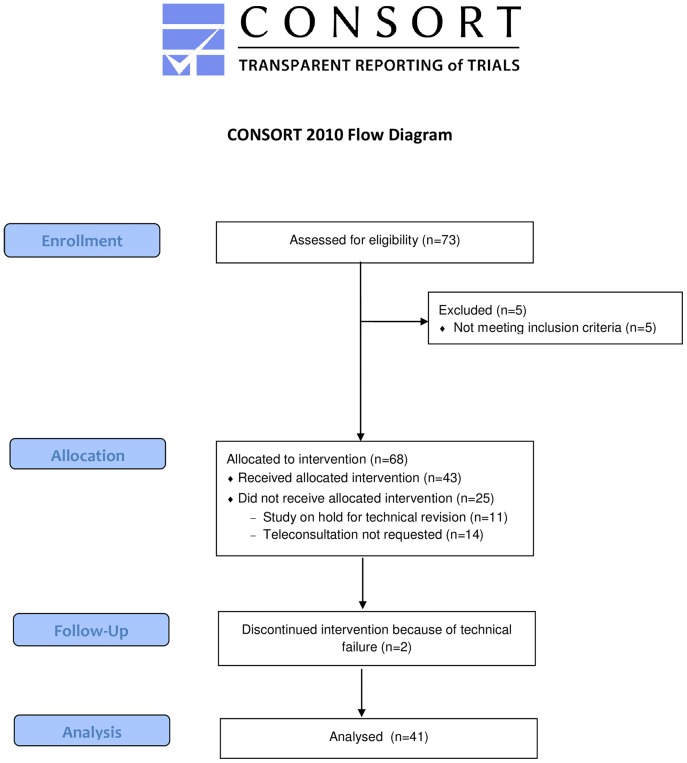
Results: Prehospital teleconsultation was obtained in 41 out of 43 cases (95.3%). The success rates for communication of blood pressure, heart rate, blood oxygen saturation, glycemia, and electronic patient identification were 78.7%, 84.8%, 80.6%, 64.0%, and 84.2%. A preliminary prehospital diagnosis was formulated in 90.2%, with satisfactory agreement with final in-hospital diagnoses. Communication of a prehospital report to the in-hospital team was successful in 94.7% and prenotification of the in-hospital team via SMS in 90.2%. Failures resulted mainly from limited mobile connectivity and to a lesser extent from software, hardware or human error. The user acceptance was high.
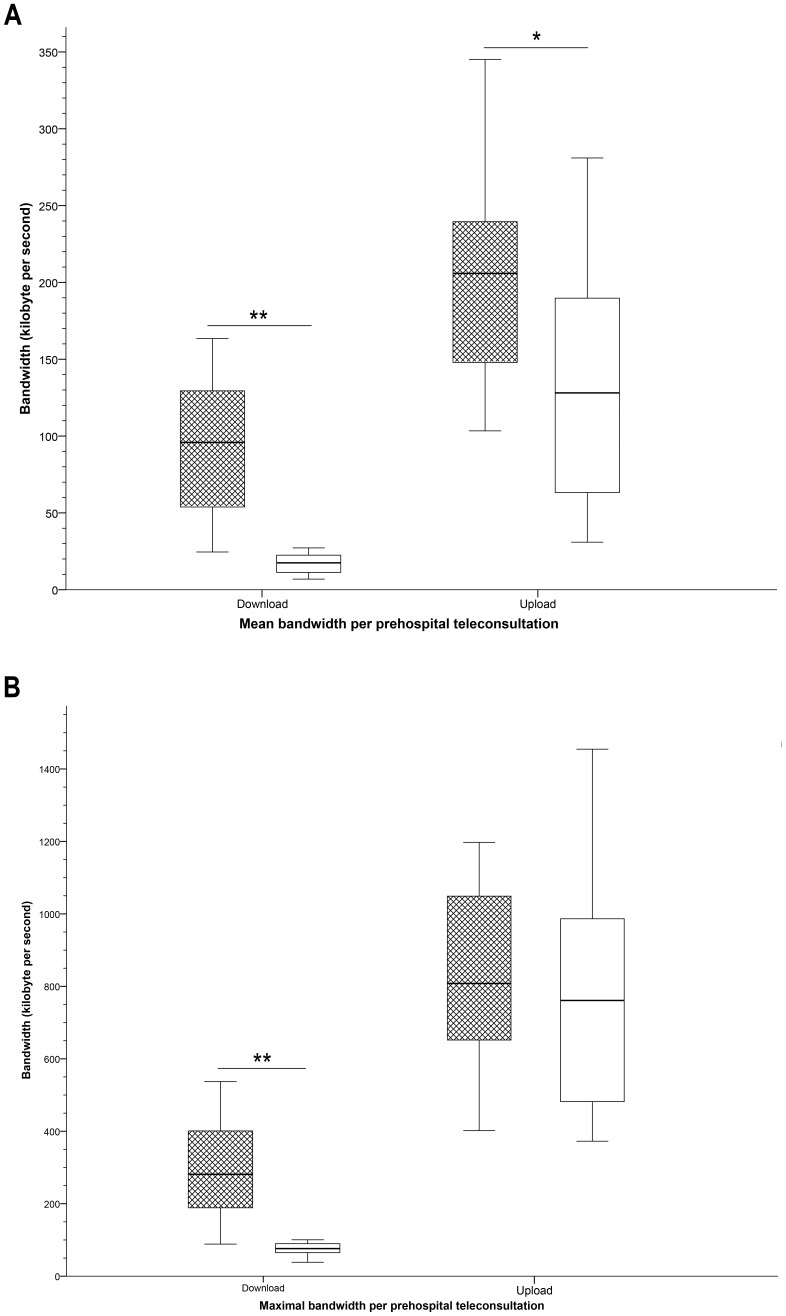
Conclusions: Ambulance-based telemedicine of the third generation is safe, feasible and reliable but further research and development, especially with regard to high speed broadband access, is needed before this approach can be implemented in daily practice.
Conflict of interest statement
Figures

References
-
- Jauch EC, Saver JL, Adams HP Jr, Bruno A, Connors JJ, et al. (2013) Guidelines for the Early Management of Patients With Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke - PubMed
-
- Hess DC, Wang S, Gross H, Nichols FT, Hall CE, et al. (2006) Telestroke: extending stroke expertise into underserved areas. Lancet Neurol 5: 275–278. - PubMed
-
- Demaerschalk BM (2011) Telemedicine or telephone consultation in patients with acute stroke. Curr Neurol Neurosci Rep 11: 42–51. - PubMed
-
- Aita MC, Nguyen K, Bacon R, Capuzzi KM (2013) Obstacles and solutions in the implementation of telestroke: billing, licensing, and legislation. Stroke 44: 3602–3606. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
