

Bacteriology and changes in antibiotic susceptibility in adults with community-acquired perforated appendicitis
- PMID: 25343342
- PMCID: PMC4208803
- DOI: 10.1371/journal.pone.0111144
Bacteriology and changes in antibiotic susceptibility in adults with community-acquired perforated appendicitis
Abstract
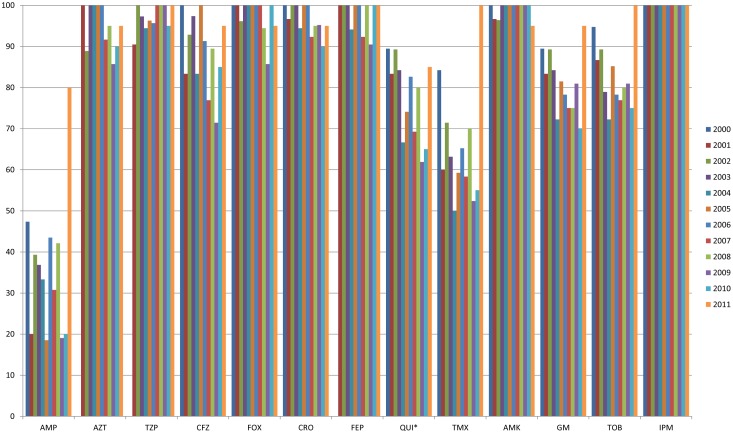
This study evaluated bacterial etiology and antibiotic susceptibility in patients diagnosed with community-acquired perforated appendicitis over a 12-year-period. We retrospectively reviewed records of adult patients diagnosed with perforated appendicitis at an 800-bed teaching hospital between January 2000 and December 2011. In total, 415 culture-positive perforated appendicitis cases were analyzed. Escherichia coli was the most common pathogen (277/415, 66.7%), followed by Streptococcus species (61/415, 14.7%). The susceptibility of E. coli to ampicillin, piperacillin/tazobactam, ceftriaxone, cefepime, amikacin, gentamicin, and imipenem was 35.1%, 97.1%, 97.0%, 98.2%, 98.9%, 81.8%, and 100%, respectively. The overall susceptibility of E. coli to quinolones (ciprofloxacin or levofloxacin) was 78.7%. During the study period, univariate logistic regression analysis showed a significant decrease in E. coli susceptibility to quinolones (OR = 0.91, 95% CI 0.84-0.99, P = 0.040). We therefore do not recommend quinolones as empirical therapy for community-acquired perforated appendicitis.
Conflict of interest statement
Figures
References
-
- Lau WY, Wong SH (1981) Randomized, prospective trial of topical hydrogen peroxide in appendectomy wound infection. High risk factors. Am J Surg 142: 393–397. - PubMed
-
- Schmit PJ, Hiyama DT, Swisher SG, Bennion RS, Thompson JE Jr (1994) Analysis of risk factors of postappendectomy intra-abdominal abscess. J Am Coll Surg 179: 721–726. - PubMed
-
- Solomkin JS, Mazuski JE, Bradley JS, Rodvold KA, Goldstein EJ, et al. (2010) Diagnosis and management of complicated intra-abdominal infection in adults and children: guidelines by the Surgical Infection Society and the Infectious Diseases Society of America. Clin Infect Dis 50: 133–164. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
