

Clinical impact of checkpoint inhibitors as novel cancer therapies
- PMID: 25344022
- PMCID: PMC4224737
- DOI: 10.1007/s40265-014-0305-6
Clinical impact of checkpoint inhibitors as novel cancer therapies
Abstract
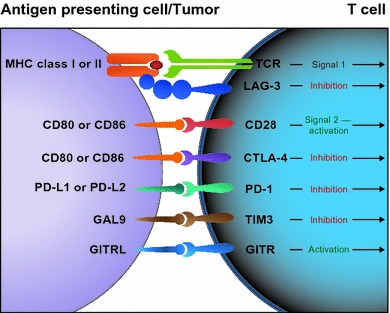
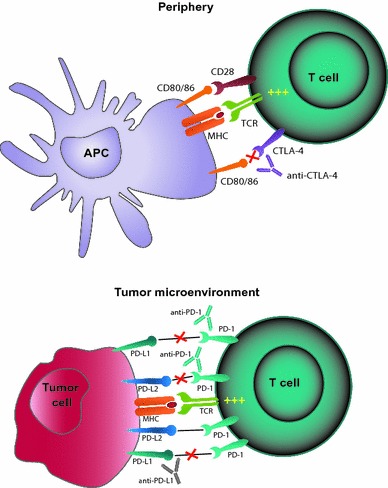
Immune responses are tightly regulated via signaling through numerous co-stimulatory and co-inhibitory molecules. Exploitation of these immune checkpoint pathways is one of the mechanisms by which tumors evade and/or escape the immune system. A growing understanding of the biology of immune checkpoints and tumor immunology has led to the development of monoclonal antibodies designed to target co-stimulatory and co-inhibitory molecules in order to re-engage the immune system and restore antitumor immune responses. Anti-cytotoxic T-lymphocyte-associated antigen 4 (CTLA-4) antibodies were among the first to be tested in the clinic, and ipilimumab was the first immune checkpoint inhibitor approved for an anticancer indication. Agents targeting the programmed death 1 (PD-1) pathway, either PD-1 or one of its ligands, programmed death ligand 1, are in active clinical development for numerous cancers, including advanced melanoma and lung cancer. Understanding the different mechanisms of action, safety profiles, and response patterns associated with inhibition of the CTLA-4 and PD-1 pathways may improve patient management as these therapies are moved in to the clinical practice setting and may also provide a rationale for combination therapy with different inhibitors. Additional immune checkpoint molecules with therapeutic potential, including lymphocyte activation gene-3 and glucocorticoid-induced tumor necrosis factor receptor-related gene, also have inhibitors in early stages of clinical development. Clinical responses and safety data reported to date on immune checkpoint inhibitors suggest these agents may have the potential to markedly improve outcomes for patients with cancer.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
