

Mechanisms of exercise intolerance in heart failure with preserved ejection fraction: the role of abnormal peripheral oxygen extraction
- PMID: 25344549
- PMCID: PMC5771713
- DOI: 10.1161/CIRCHEARTFAILURE.114.001825
Mechanisms of exercise intolerance in heart failure with preserved ejection fraction: the role of abnormal peripheral oxygen extraction
Abstract
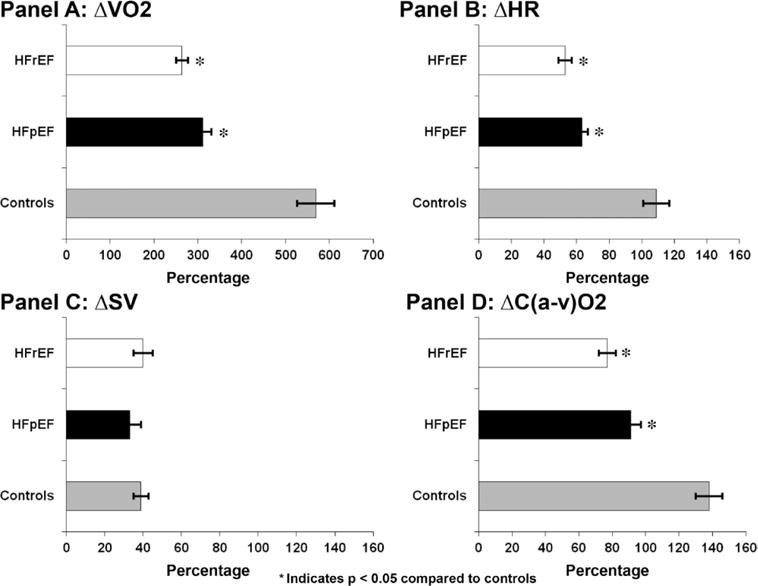
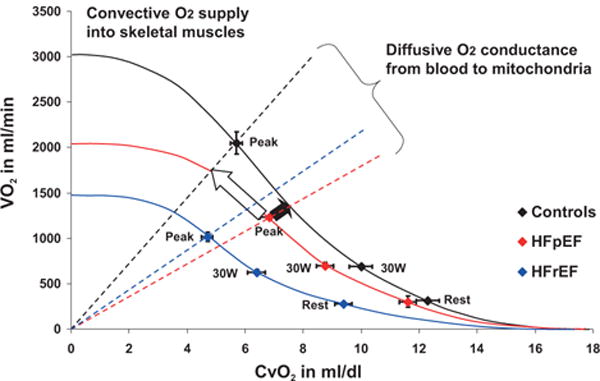
Background: Exercise capacity as measured by peak oxygen uptake (Vo2) is similarly impaired in patients with heart failure with preserved ejection fraction (HFpEF) and heart failure with reduced ejection fraction (HFrEF). However, characterization of how each component of Vo2 changes in response to incremental exercise in HFpEF versus HFrEF has not been previously defined. We hypothesized that abnormally low peripheral o2 extraction (arterio-mixed venous o2 content difference, [C(a-v)o2]) during exercise significantly contributes to impaired exercise capacity in HFpEF.
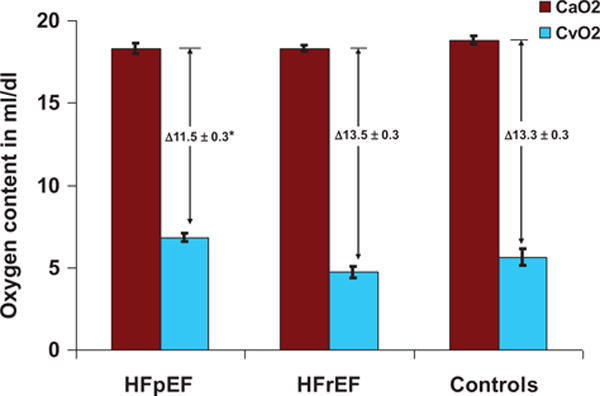
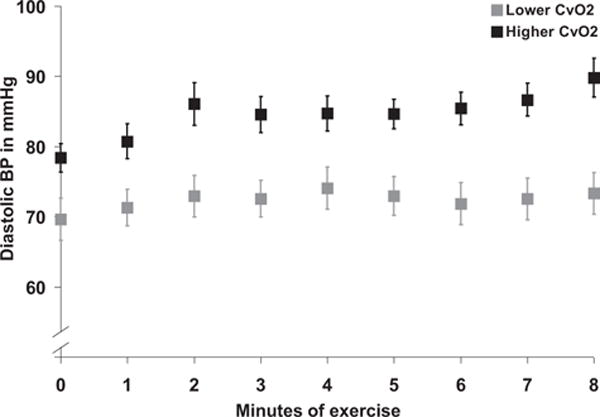
Methods and results: We performed maximum incremental cardiopulmonary exercise testing with invasive hemodynamic monitoring on 104 patients with symptomatic NYHA II to IV heart failure (HFpEF, n=48, peak Vo2=13.9±0.5 mL kg(-1) min(-1), mean±SEM, and HFrEF, n=56, peak Vo2=12.1±0.5 mL kg(-1) min(-1)) and 24 control subjects (peak Vo2 27.0±1.7 mL kg(-1) min(-1)). Peak exercise C(a-v)o2 was lower in HFpEF compared with HFrEF (11.5±0.27 versus 13.5±0.34 mL/dL, respectively, P<0.0001), despite no differences in age, hemoglobin level, peak respiratory exchange ratio, Cao2, or cardiac filling pressures. Peak C(a-v)o2 and peak heart rate emerged as the leading predictors of peak Vo2 in HFpEF. Impaired peripheral o2 extraction was the predominant limiting factor to exercise capacity in 40% of patients with HFpEF and was closely related to elevated systemic blood pressure during exercise (r=0.49, P=0.0005).
Conclusions: In the first study to directly measure C(a-v)o2 throughout exercise in HFpEF, HFrEF, and normals, we found that peak C(a-v)o2 was a major determinant of exercise capacity in HFpEF. The important functional limitation imposed by impaired o2 extraction may reflect intrinsic abnormalities in skeletal muscle or peripheral microvascular function, and represents a potential target for therapeutic intervention.
Keywords: diastole; exercise; heart failure.
© 2014 American Heart Association, Inc.
Figures
Comment in
-
Exercise intolerance in heart failure with preserved ejection fraction: what does the heart have to do with it?Circ Heart Fail. 2015 Mar;8(2):233-5. doi: 10.1161/CIRCHEARTFAILURE.114.001966. Circ Heart Fail. 2015. PMID: 25783946 No abstract available.
Similar articles
-
Impaired oxygen uptake kinetics in heart failure with preserved ejection fraction.Heart. 2019 Oct;105(20):1552-1558. doi: 10.1136/heartjnl-2019-314797. Epub 2019 Jun 17. Heart. 2019. PMID: 31208971
-
Differential Responses of Post-Exercise Recovery of Leg Blood Flow and Oxygen Uptake Kinetics in HFpEF versus HFrEF.PLoS One. 2016 Oct 4;11(10):e0163513. doi: 10.1371/journal.pone.0163513. eCollection 2016. PLoS One. 2016. PMID: 27701422 Free PMC article.
-
Determinants of Effort Intolerance in Patients With Heart Failure: Combined Echocardiography and Cardiopulmonary Stress Protocol.JACC Heart Fail. 2015 Oct;3(10):803-14. doi: 10.1016/j.jchf.2015.05.010. JACC Heart Fail. 2015. PMID: 26449998
-
Mechanisms of the Improvement in Peak VO2 With Exercise Training in Heart Failure With Reduced or Preserved Ejection Fraction.Heart Lung Circ. 2018 Jan;27(1):9-21. doi: 10.1016/j.hlc.2017.07.002. Epub 2017 Aug 4. Heart Lung Circ. 2018. PMID: 28870770 Review.
-
Determinants of exercise intolerance in patients with heart failure and reduced or preserved ejection fraction.J Appl Physiol (1985). 2015 Sep 15;119(6):739-44. doi: 10.1152/japplphysiol.00049.2015. Epub 2015 Apr 24. J Appl Physiol (1985). 2015. PMID: 25911681 Free PMC article. Review.
Cited by
-
Cardiovascular Functional Changes in Chronic Kidney Disease: Integrative Physiology, Pathophysiology and Applications of Cardiopulmonary Exercise Testing.Front Physiol. 2020 Sep 15;11:572355. doi: 10.3389/fphys.2020.572355. eCollection 2020. Front Physiol. 2020. PMID: 33041870 Free PMC article. Review.
-
Percent Predicted Peak Exercise Oxygen Pulse Provides Insights Into Ventricular-Vascular Response and Prognosticates HFpEF.JACC Adv. 2024 Jul 12;3(8):101101. doi: 10.1016/j.jacadv.2024.101101. eCollection 2024 Aug. JACC Adv. 2024. PMID: 39105119 Free PMC article.
-
Pulmonary Vascular Distensibility Predicts Pulmonary Hypertension Severity, Exercise Capacity, and Survival in Heart Failure.Circ Heart Fail. 2016 Jun;9(6):10.1161/CIRCHEARTFAILURE.115.003011 e003011. doi: 10.1161/CIRCHEARTFAILURE.115.003011. Circ Heart Fail. 2016. PMID: 27301469 Free PMC article. Clinical Trial.
-
Cardiopulmonary exercise testing and echocardiographic exam: an useful interaction.Cardiovasc Ultrasound. 2019 Dec 3;17(1):29. doi: 10.1186/s12947-019-0180-0. Cardiovasc Ultrasound. 2019. PMID: 31796047 Free PMC article. Review.
-
Unexplained exertional intolerance associated with impaired systemic oxygen extraction.Eur J Appl Physiol. 2019 Oct;119(10):2375-2389. doi: 10.1007/s00421-019-04222-6. Epub 2019 Sep 6. Eur J Appl Physiol. 2019. PMID: 31493035
References
-
- Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med. 2006;355:251–259. - PubMed
-
- Paulus WJ, Tschöpe C, Sanderson JE, Rusconi C, Flachskampf FA, Rademakers FE, Marino P, Smiseth OA, De Keulenaer G, Leite-Moreira AF, Borbély A, Edes I, Handoko ML, Heymans S, Pezzali N, Pieske B, Dickstein K, Fraser AG, Brutsaert DL. How to diagnose diastolic heart failure: a consensus statement on the diagnosis of heart failure with normal left ventricular ejection fraction by the Heart Failure and Echocardiography Associations of the European Society of Cardiology. Eur Heart J. 2007;28:2539–2550. - PubMed
-
- Kitzman DW, Little WC, Brubaker PH, Anderson RT, Hundley WG, Marburger CT, Brosnihan B, Morgan TM, Stewart KP. Pathophysiological characterization of isolated diastolic heart failure in comparison to systolic heart failure. JAMA. 2002;288:2144–2150. - PubMed
-
- Tribouilloy C, Rusinaru D, Mahjoub H, Soulière V, Lévy F, Peltier M, Slama M, Massy Z. Prognosis of heart failure with preserved ejection fraction: a 5 year prospective population-based study. Eur Heart J. 2008;29:339–347. - PubMed
-
- Kitzman DW, Higginbotham MB, Cobb FR, Sheikh KH, Sullivan MJ. Exercise intolerance in patients with heart failure and preserved left ventricular systolic function: failure of the Frank-Starling mechanism. J Am Coll Cardiol. 1991;17:1065–1072. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
