

Common patterns of morbidity and multi-morbidity and their impact on health-related quality of life: evidence from a national survey
- PMID: 25344816
- PMCID: PMC4366552
- DOI: 10.1007/s11136-014-0820-7
Common patterns of morbidity and multi-morbidity and their impact on health-related quality of life: evidence from a national survey
Abstract
Background: There is limited evidence about the impact of specific patterns of multi-morbidity on health-related quality of life (HRQoL) from large samples of adult subjects.
Methods: We used data from the English General Practice Patient Survey 2011-2012. We defined multi-morbidity as the presence of two or more of 12 self-reported conditions or another (unspecified) long-term health problem. We investigated differences in HRQoL (EQ-5D scores) associated with combinations of these conditions after adjusting for age, gender, ethnicity, socio-economic deprivation and the presence of a recent illness or injury. Analyses were based on 831,537 responses from patients aged 18 years or older in 8,254 primary care practices in England.
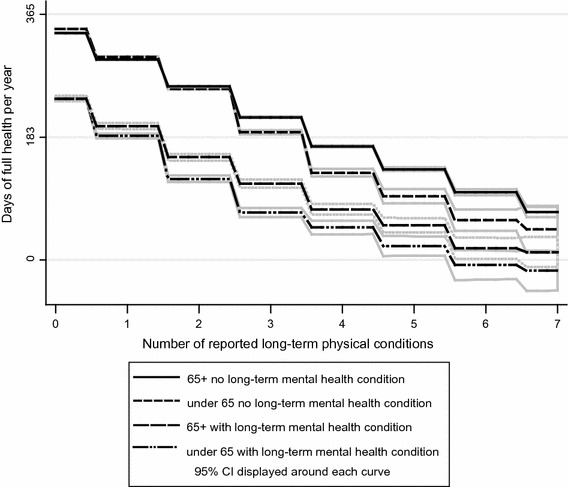
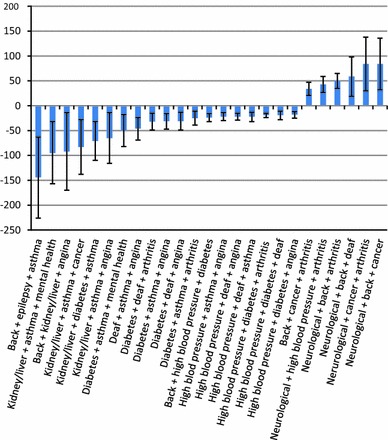
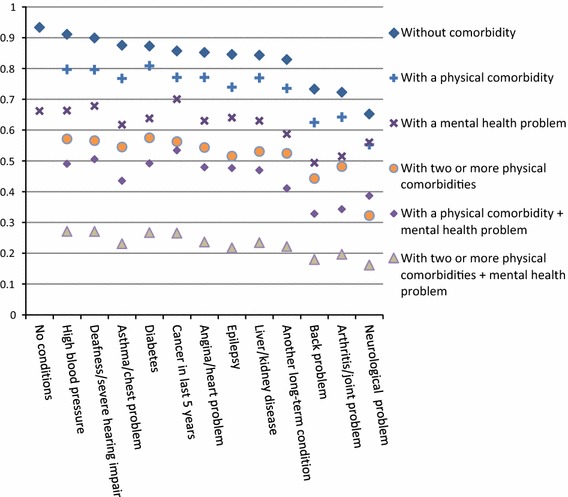
Results: Of respondents, 23 % reported two or more chronic conditions (ranging from 7 % of those under 45 years of age to 51 % of those 65 years or older). Multi-morbidity was more common among women, White individuals and respondents from socio-economically deprived areas. Neurological problems, mental health problems, arthritis and long-term back problem were associated with the greatest HRQoL deficits. The presence of three or more conditions was commonly associated with greater reduction in quality of life than that implied by the sum of the differences associated with the individual conditions. The decline in quality of life associated with an additional condition in people with two and three physical conditions was less for older people than for younger people. Multi-morbidity was associated with a substantially worse HRQoL in diabetes than in other long-term conditions. With the exception of neurological conditions, the presence of a comorbid mental health problem had a more adverse effect on HRQoL than any single comorbid physical condition.
Conclusion: Patients with multi-morbid diabetes, arthritis, neurological, or long-term mental health problems have significantly lower quality of life than other people. People with long-term health conditions require integrated mental and physical healthcare services.
Figures
References
-
- Saarni SI, Harkanen T, Sintonen H, Suvisaari J, Koskinen S, Aromaa A, Lonnqvist J. The impact of 29 chronic conditions on health-related quality of life: A general population survey in Finland using 15D and EQ-5D. Quality of Life Research. 2006;15(8):1403–1414. doi: 10.1007/s11136-006-0020-1. - DOI - PubMed
-
- Brettschneider C, Leicht H, Bickel H, Dahlhaus A, Fuchs A, Gensichen J, et al. (MultiCare Study Group). Relative impact of multimorbid chronic conditions on health-related quality of life–results from the MultiCare Cohort Study. PLoS One. 2013;8(6):e66742. doi: 10.1371/journal.pone.0066742. - DOI - PMC - PubMed
-
- Alonso J, Ferrer M, Gandek B, Ware JE, Jr, Aaronson NK, Mosconi P, Rasmussen NK, Bullinger M, Fukuhara S, Kaasa S, Leplege A. Health-related quality of life associated with chronic conditions in eight countries: Results from the International Quality of Life Assessment (IQOLA) Project. Quality of Life Research. 2004;13(2):283–298. doi: 10.1023/B:QURE.0000018472.46236.05. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
