

Glycogen synthase kinase-3β inhibition depletes the population of prostate cancer stem/progenitor-like cells and attenuates metastatic growth
- PMID: 25344861
- PMCID: PMC4253412
- DOI: 10.18632/oncotarget.1510
Glycogen synthase kinase-3β inhibition depletes the population of prostate cancer stem/progenitor-like cells and attenuates metastatic growth
Abstract
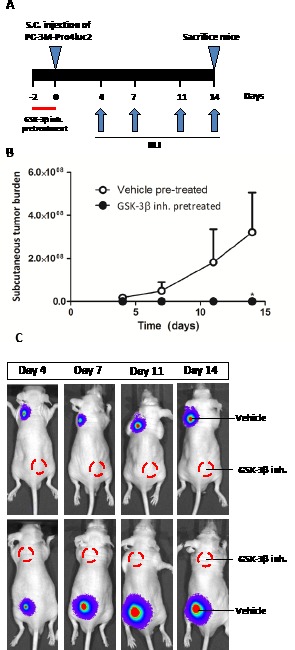
Cancer cells with stem or progenitor properties play a pivotal role in the initiation, recurrence and metastatic potential of solid tumors, including those of the human prostate. Cancer stem cells are generally more resistant to conventional therapies thus requiring the characterization of key pathways involved in the formation and/or maintenance of this malignant cellular subpopulation. To this end, we identified Glycogen Synthase Kinase-3β (GSK-3β) as a crucial kinase for the maintenance of prostate cancer stem/progenitor-like cells and pharmacologic inhibition of GSK-3β dramatically decreased the size of this cellular subpopulation. This was paralleled by impaired clonogenicity, decreased migratory potential and dramatic morphological changes. In line with our in vitro observations, treatment with a GSK-3β inhibitor leads to a complete loss of tumorigenicity and a decrease in metastatic potential in preclinical in vivo models. These observed anti-tumor effects appear to be largely Wnt-independent as simultaneous Wnt inhibition does not reverse the observed antitumor effects of GSK-3β blockage. We found that GSK-3β activity is linked to cytoskeletal protein F-actin and inhibition of GSK-3β leads to disturbance of F-actin polymerization. This may underlie the dramatic effects of GSK-3β inhibition on prostate cancer migration. Furthermore, GSK-3β inhibition led to strongly decreased expression of several integrin types including the cancer stem cell-associated α2β1 integrin. Taken together, our mechanistic observations highlight the importance of GSK-3β activity in prostate cancer stemness and may facilitate the development of novel therapy for advanced prostate cancer.
Conflict of interest statement
The authors declare no conflict of interest.
Figures




References
-
- Jemal A, Center MM, DeSantis C, Ward EM. Global patterns of cancer incidence and mortality rates and trends. Cancer Epidemiol Biomarkers Prev. 2010;19(8):1893–1907. - PubMed
-
- Wirth MP, See WA, McLeod DG, Iversen P, Morris T, Carroll K, Casodex Early Prostate Cancer Trialists G Bicalutamide 150 mg in addition to standard care in patients with localized or locally advanced prostate cancer: results from the second analysis of the early prostate cancer program at median followup of 5. 4 years. J Urol. 2004;172(5 Pt 1):1865–1870. - PubMed
-
- Petrylak DP, Tangen CM, Hussain MH, Lara PN, Jr, Jones JA, Taplin ME, Burch PA, Berry D, Moinpour C, Kohli M, Benson MC, Small EJ, Raghavan D, Crawford ED. Docetaxel and estramustine compared with mitoxantrone and prednisone for advanced refractory prostate cancer. N Engl J Med. 2004;351(15):1513–1520. - PubMed
-
- Tannock IF, de Wit R, Berry WR, Horti J, Pluzanska A, Chi KN, Oudard S, Theodore C, James ND, Turesson I, Rosenthal MA, Eisenberger MA, Investigators TAX. Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer. N Engl J Med. 2004;351(15):1502–1512. - PubMed
-
- Attard G, Reid AH, Yap TA, Raynaud F, Dowsett M, Settatree S, Barrett M, Parker C, Martins V, Folkerd E, Clark J, Cooper CS, Kaye SB, Dearnaley D, Lee G, de Bono JS. Phase I clinical trial of a selective inhibitor of CYP17, abiraterone acetate, confirms that castration-resistant prostate cancer commonly remains hormone driven. J Clin Oncol. 2008;26(28):4563–4571. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
