

Horizontal Resorption of Fresh-Frozen Corticocancellous Bone Blocks in the Reconstruction of the Atrophic Maxilla at 5 Months
- PMID: 25346211
- PMCID: PMC4616242
- DOI: 10.1111/cid.12268
Horizontal Resorption of Fresh-Frozen Corticocancellous Bone Blocks in the Reconstruction of the Atrophic Maxilla at 5 Months
Abstract
Background: Reliable implant-supported rehabilitation of an alveolar ridge needs sufficient volume of bone. In order to achieve a prosthetic-driven positioning, bone graft techniques may be required.
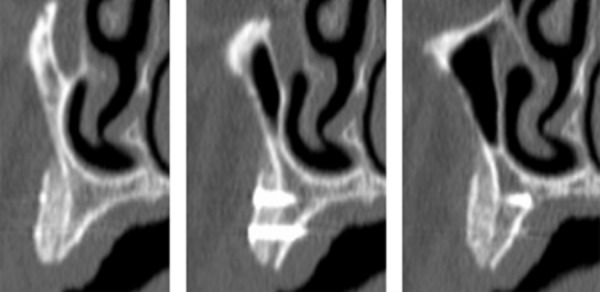
Purpose: This prospective cohort study aims to clinically evaluate the amount of resorption of corticocancellous fresh-frozen allografts bone blocks used in the reconstruction of the severe atrophic maxilla.
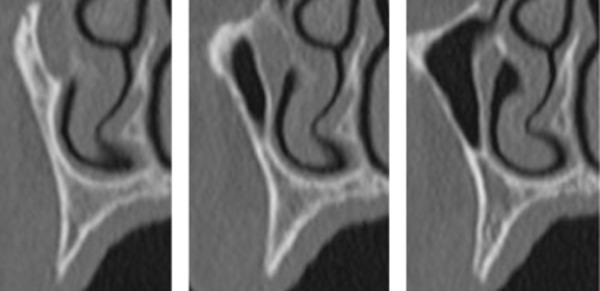
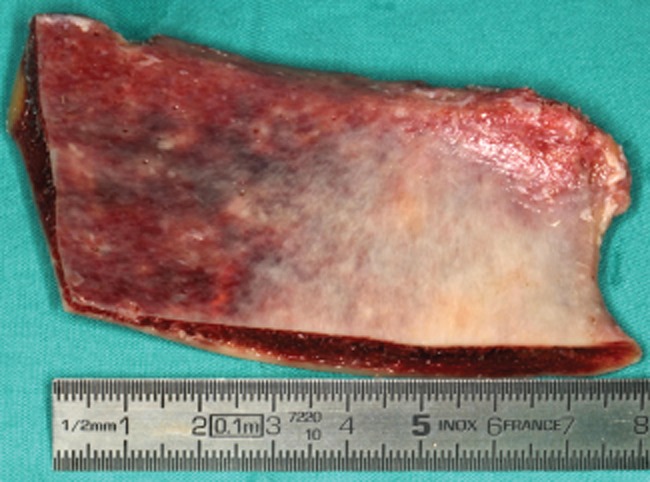
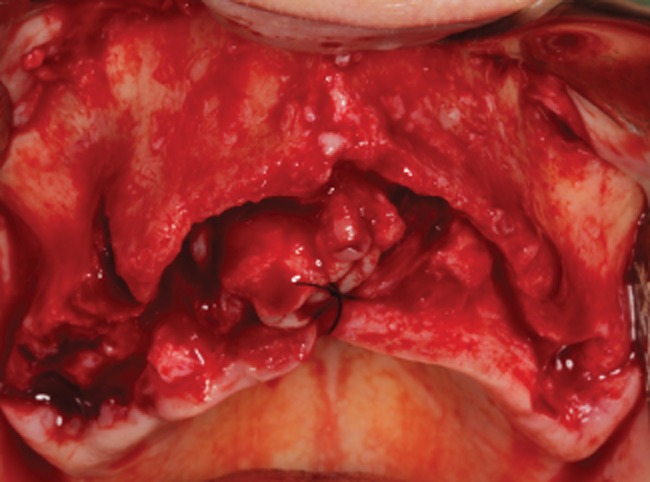
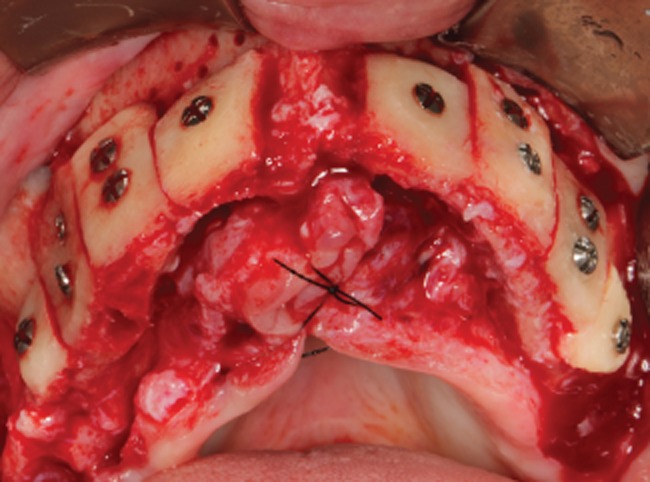
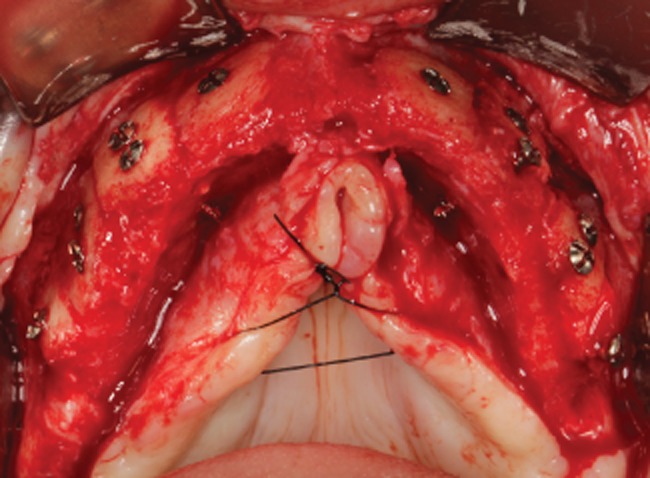
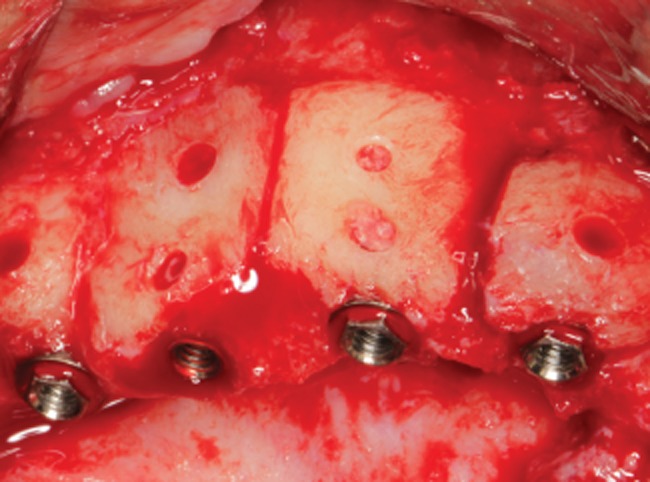
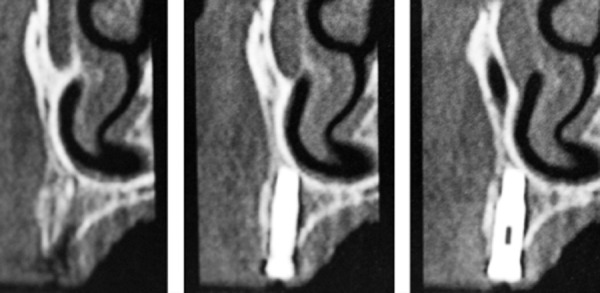
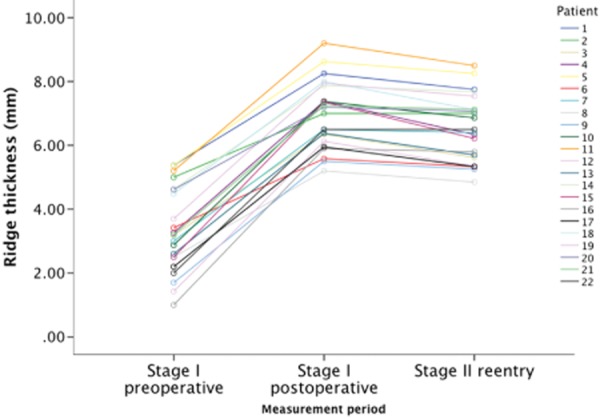
Materials and methods: Twenty-two partial and totally edentulous patients underwent bone augmentation procedures with fresh-frozen allogenous blocks from the iliac crest under local anesthesia. Implants were inserted into the grafted sites after a healing period of 5 months. Final fixed prosthesis was delivered ± 4 months later. Ridge width analysis and measurements were performed with a caliper before and after grafting and at implant insertion. Bone biopsies were performed in 16 patients.
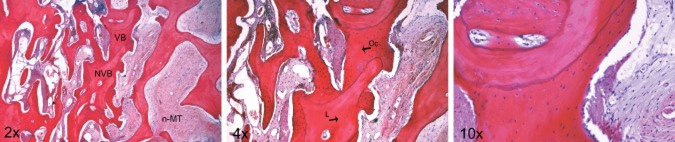
Results: A total of 98 onlay block allografts were used in 22 patients with an initial mean alveolar ridge width of 3.41 ± 1.36 mm. Early exposure of blocks was observed in four situations and one of these completely resorbed. Mean horizontal bone gain was 3.63 ± 1.28 mm (p < .01). Mean buccal bone resorption between allograph placement and the reopening stage was 0.49 ± 0.54 mm, meaning approximately 7.1% (95% confidence interval: [5.6%, 8.6%]) of total ridge width loss during the integration period. One hundred thirty dental implants were placed with good primary stability (≥ 30 Ncm). Four implants presented early failure before the prosthetic delivery (96.7% implant survival). All patients were successfully rehabilitated. Histomorphometric analysis revealed 20.9 ± 5.8% of vital bone in close contact to the remaining grafted bone. A positive strong correlation (adjusted R(2) = 0.44, p = .003) was found between healing time and vital bone percentage.
Conclusions: Augmentation procedures performed using fresh-frozen allografts from the iliac crest are a suitable alternative in the reconstruction of the atrophic maxilla with low resorption rate at 5 months, allowing proper stability of dental implants followed by fixed prosthetic rehabilitation.
Keywords: allografts; alveolar ridge augmentation; corticocancellous block; fresh-frozen bone; iliac crest.
© 2014 Wiley Periodicals, Inc.
Figures


Similar articles
-
Maxillary alveolar ridge reconstruction with nonvascularized autogenous block bone: clinical results.J Oral Maxillofac Surg. 2007 Oct;65(10):2039-46. doi: 10.1016/j.joms.2007.05.017. J Oral Maxillofac Surg. 2007. PMID: 17884536 Clinical Trial.
-
A new technique for reconstruction of the atrophied narrow alveolar crest in the maxilla using morselized impacted bone allograft and later placement of dental implants.Clin Implant Dent Relat Res. 2008 May;10(2):86-92. doi: 10.1111/j.1708-8208.2007.00063.x. Clin Implant Dent Relat Res. 2008. PMID: 18462204
-
Deep-frozen allogeneic onlay bone grafts for reconstruction of atrophic maxillary alveolar ridges: a preliminary study.J Oral Maxillofac Surg. 2009 Jun;67(6):1300-6. doi: 10.1016/j.joms.2008.12.043. J Oral Maxillofac Surg. 2009. PMID: 19446220
-
Implant reconstruction of the bone-grafted maxilla: review of the literature and presentation of 8 cases.J Oral Maxillofac Surg. 2006 Apr;64(4):674-82. doi: 10.1016/j.joms.2005.12.026. J Oral Maxillofac Surg. 2006. PMID: 16546648 Review.
-
Managing the Posterior Maxilla with Implants Using Bone Grafting to Enhance Implant Sites.Oral Maxillofac Surg Clin North Am. 2019 May;31(2):299-308. doi: 10.1016/j.coms.2019.01.002. Epub 2019 Mar 7. Oral Maxillofac Surg Clin North Am. 2019. PMID: 30852176 Review.
Cited by
-
Collagenated Porcine Heterologous Bone Grafts: Histomorphometric Evaluation of Bone Formation Using Different Physical Forms in a Rabbit Cancellous Bone Model.Molecules. 2021 Mar 2;26(5):1339. doi: 10.3390/molecules26051339. Molecules. 2021. PMID: 33801547 Free PMC article.
-
Volumetric Changes of a Customized Allogeneic Bone Block Measured by Two Image Matching Tools: Introduction of a Novel Assessment Technique for Graft Resorption.Acta Stomatol Croat. 2021 Dec;55(4):406-417. doi: 10.15644/asc55/4/8. Acta Stomatol Croat. 2021. PMID: 35001936 Free PMC article.
-
Design Techniques to Optimize the Scaffold Performance: Freeze-dried Bone Custom-made Allografts for Maxillary Alveolar Horizontal Ridge Augmentation.Materials (Basel). 2020 Mar 19;13(6):1393. doi: 10.3390/ma13061393. Materials (Basel). 2020. PMID: 32204393 Free PMC article.
-
Dental Implant Placement with Simultaneous Anterior Maxillary Reconstruction with Block and Particulate Fresh Frozen Allograft Bone: A Case Report with 24-Month Follow-Up Data.Case Rep Surg. 2017;2017:1565973. doi: 10.1155/2017/1565973. Epub 2017 Feb 16. Case Rep Surg. 2017. PMID: 28299226 Free PMC article.
-
Comparison of allogeneic and autogenous bone grafts for augmentation of alveolar ridge defects-A 12-month retrospective radiographic evaluation.Clin Oral Implants Res. 2018 Nov;29(11):1163-1175. doi: 10.1111/clr.13380. Epub 2018 Oct 31. Clin Oral Implants Res. 2018. PMID: 30303581 Free PMC article.
References
-
- Tallgren A. The continuing reduction of the residual alveolar ridges in complete denture wearers: A mixed-longitudinal study covering 25 years. J Prosthet Dent. 2003;89(5):427–435. - PubMed
-
- Cardaropoli G, Araújo M, Hayacibara R, Sukekava F, Lindhe J. Healing of extraction sockets and surgically produced - augmented and non-augmented - defects in the alveolar ridge. An experimental study in the dog. J Clin Periodontol. 2005;32:435–440. - PubMed
-
- Cawood JI, Howell RA. A classification of the edentulous jaws. Int J Oral Maxillofac Surg. 1988;17(4):232–236. - PubMed
-
- Schropp L, Wenzel A, Kostopoulos L, Karring T. Bone healing and soft tissue contour changes following single-tooth extraction: a clinical and radiographic 12-month prospective study. Int J Periodontics Restorative Dent. 2003;23(4):313–323. - PubMed
-
- Nevins M, Camelo M, De Paoli S, Friedland B, Schenk RK, Parma-Benfenati S, et al. A study of the fate of the buccal wall of extraction sockets of teeth with prominent roots. Int J Periodontics Restorative Dent. 2006;26(1):19–29. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
