

The treatment of chronic recurrent oral aphthous ulcers
- PMID: 25346356
- PMCID: PMC4215084
- DOI: 10.3238/arztebl.2014.0665
The treatment of chronic recurrent oral aphthous ulcers
Abstract
Background: Chronic recurrent oral aphthous ulcers are the most common type of inflammatory efflorescence of the oral mucosa, with a prevalence of 2% to 10% in Caucasian populations. To treat them properly, physicians should know their clinical appearance and course, conditioning factors, underlying causes, and differential diagnosis.
Method: This review is based on pertinent articles that were retrieved by a selective search in PubMed and in the Cochrane Central Register of Controlled Trials.
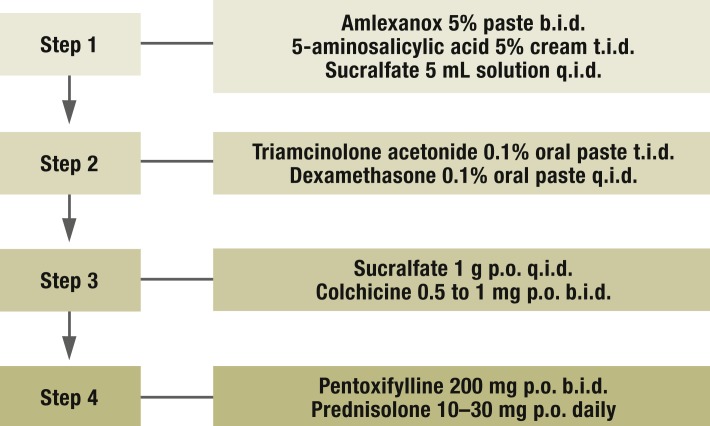
Results: Hard, acidic, and salty foods and toothpastes containing sodium lauryl sulfate should be avoided, along with alcohol and carbonated drinks. In Germany, the only drugs that have been approved to treat oral aphthous ulcers are corticosteroids, topical antiseptic/anti-inflammatory agents such as triclosan and diclofenac, and local anesthetics such as lidocaine. Antiseptic agents and local anesthetics should be tried first; if these are ineffective, topical cortico steroids should be used. In severe cases, local measures can be combined with systemic drugs, e.g., colchicine, pentoxifylline, or prednisolone. The efficacy of systemic treatment is debated. Other immunosuppressive agents should be given systemically only for refractory or particularly severe oral aphthous ulcers due to Adamantiades-Behçet disease.
Conclusion: The treatment of chronic recurrent oral aphthous ulcers is symptomatic, mainly with topically applied agents. It is tailored to the severity of the problem in the individual case, i.e., the frequency of ulcers, the intensity of pain, and the responsiveness of the lesions to treatment. Effective treatment relieves pain, lessens functional impairment, and lowers the frequency and severity of recurrences.
Figures

Comment in
-
Fumaric acid esters as an additional systemic therapy option.Dtsch Arztebl Int. 2015 Mar 27;112(13):222. doi: 10.3238/arztebl.2015.0222a. Dtsch Arztebl Int. 2015. PMID: 25869344 Free PMC article. No abstract available.
-
Acatalasia was omitted.Dtsch Arztebl Int. 2015 Mar 27;112(13):222. doi: 10.3238/arztebl.2015.0222b. Dtsch Arztebl Int. 2015. PMID: 25869345 Free PMC article. No abstract available.
-
In reply.Dtsch Arztebl Int. 2015 Mar 27;112(13):222-3. doi: 10.3238/arztebl.2015.0222c. Dtsch Arztebl Int. 2015. PMID: 25869346 Free PMC article. No abstract available.
References
-
- Altenburg A, Krahl D, Zouboulis CC. Nicht-infektiöse exulzerierende Mundschleimhauterkrankungen. J Dtsch Dermatol Ges. 2008;7:242–257. - PubMed
-
- Bork K, Burgdorf W, Hoede N. 3rd. Stuttgart: Schattauer; 2008. Mundschleimhaut und Lippenkrankheiten; pp. 49–58.
-
- Rogers RS. Complex aphthosis. Adv Exp Med Biol. (3rd) 2003;528:311–316. - PubMed
-
- Hornstein OP. Aphthen und aphthoide Läsionen der Mundschleimhaut. HNO. 1998;46:102–111. - PubMed
-
- Kleinman DV, Swango PA, Pindborg JJ. Epidemiology of oral mucosal lesions in United States schoolchildren: 1986-87. Community Dent Oral Epidemiol. 1994;22:243–253. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical