

A decision support tool for appropriate glucose-lowering therapy in patients with type 2 diabetes
- PMID: 25347226
- PMCID: PMC4346378
- DOI: 10.1089/dia.2014.0260
A decision support tool for appropriate glucose-lowering therapy in patients with type 2 diabetes
Abstract
Background: Optimal glucose-lowering therapy in type 2 diabetes mellitus requires a patient-specific approach. Although a good framework, current guidelines are insufficiently detailed to address the different phenotypes and individual needs of patients seen in daily practice. We developed a patient-specific decision support tool based on a systematic analysis of expert opinion.
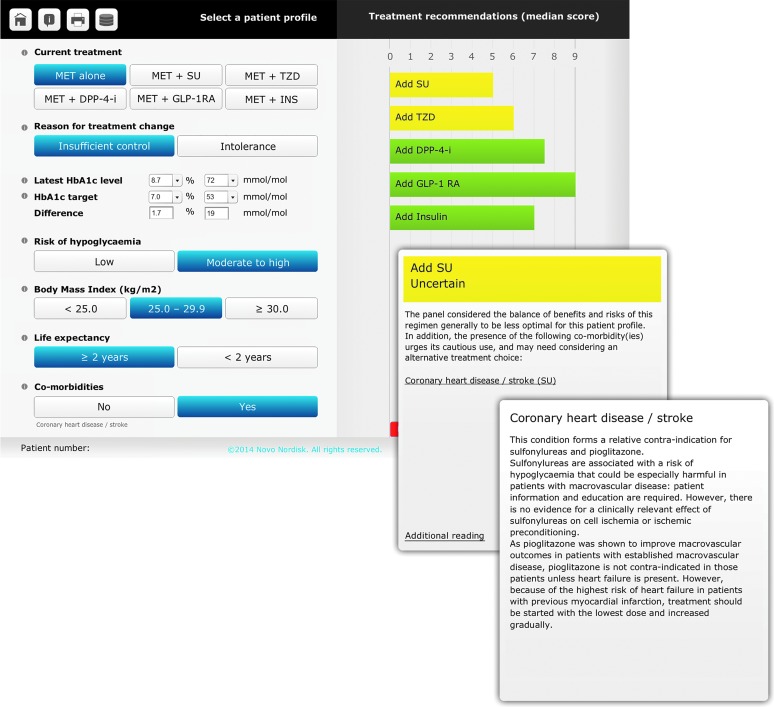
Materials and methods: Based on the American Diabetes Association (ADA)/European Association for the Study of Diabetes (EASD) 2012 position statement, a panel of 12 European experts rated the appropriateness (RAND/UCLA Appropriateness Method) of treatment strategies for 930 clinical scenarios, which were permutations of clinical variables considered relevant to treatment choice. These included current treatment, hemoglobin A1c difference from individualized target, risk of hypoglycemia, body mass index, life expectancy, and comorbidities. Treatment options included addition of a second or third agent, drug switches, and replacement by monotherapies if the patient was metformin-intolerant. Treatment costs were not considered. Appropriateness (appropriate, inappropriate, uncertain) was based on the median score and expert agreement. The panel recommendations were embedded in an online decision support tool (DiaScope(®); Novo Nordisk Health Care AG, Zürich, Switzerland).
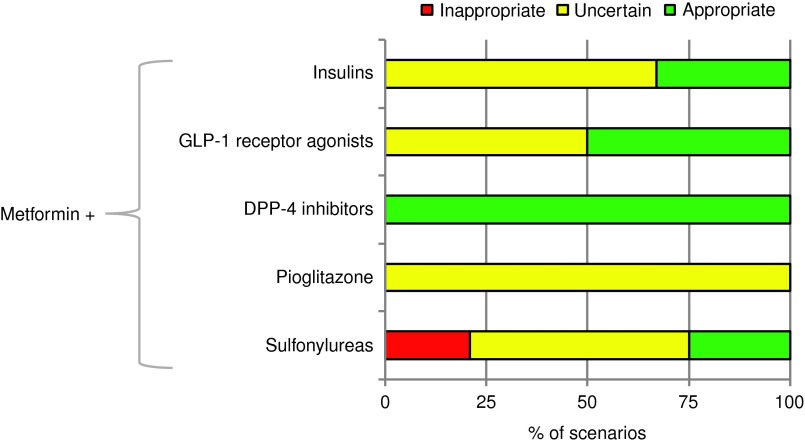
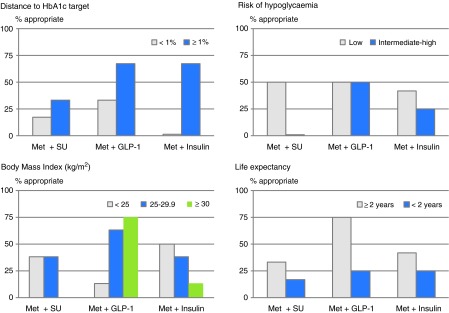
Results: Treatment appropriateness was associated with (combinations of) the patient variables mentioned above. As second-line agents, dipeptidyl peptidase-4 inhibitors were considered appropriate in all scenarios, followed by glucagon-like peptide-1 receptor agonists (50%), insulins (33%), and sulfonylureas (25%), but not pioglitazone (0%). Ratings of third-line combinations followed a similar pattern. Disagreement was highest for regimens including pioglitazone, sulfonylureas, or insulins and was partly due to differences in panelists' opinions and in drug availability and reimbursement across European countries (although costs were disregarded in the rating process).
Conclusions: A novel decision support tool based on the ADA/EASD 2012 position statement and a systematic analysis of expert opinion has been developed to help healthcare professionals to individualize glucose-lowering therapy in daily clinical situations.
Figures
References
-
- Inzucchi SE, Bergenstal RM, Buse JB, et al. : Management of hyperglycemia in type 2 diabetes: a patient-centered approach. Position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia 2012;55:1577–1596 - PubMed
-
- Turnbull FM, Abraira C, Anderson RJ, et al. : Intensive glucose control and macrovascular outcomes in type 2 diabetes. Diabetologia 2009;52:2288–2298 - PubMed
-
- Scirica BM, Bhatt DL, Braunwald E, et al. : Saxagliptin and cardiovascular outcomes in patients with type 2 diabetes mellitus. N Engl J Med 2013;369:1317–1326 - PubMed
-
- White WB, Cannon CP, Heller SR, et al. : Alogliptin after acute coronary syndrome in patients with type 2 diabetes. N Engl J Med 2013;369:1327–1335 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials