

Association of opioid agonist therapy with lower incidence of hepatitis C virus infection in young adult injection drug users
- PMID: 25347412
- PMCID: PMC4506774
- DOI: 10.1001/jamainternmed.2014.5416
Association of opioid agonist therapy with lower incidence of hepatitis C virus infection in young adult injection drug users
Abstract
Importance: Injection drug use is the primary mode of transmission for hepatitis C virus (HCV) infection. Prior studies suggest opioid agonist therapy may reduce the incidence of HCV infection among injection drug users; however, little is known about the effects of this therapy in younger users.
Objective: To evaluate whether opioid agonist therapy was associated with a lower incidence of HCV infection in a cohort of young adult injection drug users.
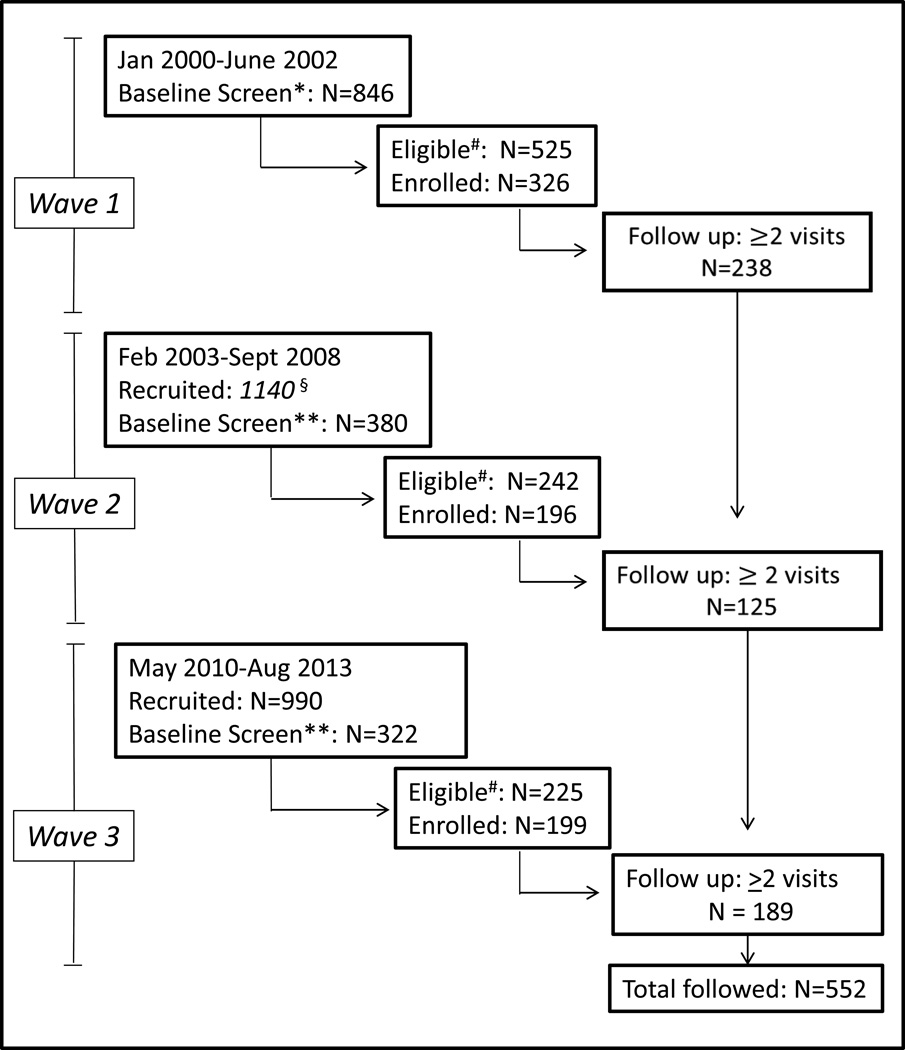
Design, setting, and participants: Observational cohort study conducted from January 3, 2000, through August 21, 2013, with quarterly interviews and blood sampling. We recruited young adult (younger than 30 years) injection drug users who were negative for anti-HCV antibody and/or HCV RNA.
Exposures: Substance use treatment within the past 3 months, including non-opioid agonist forms of treatment, opioid agonist (methadone hydrochloride or buprenorphine hydrochloride) detoxification or maintenance therapy, or no treatment.
Main outcomes and measures: Incident HCV infection documented with a new positive result for HCV RNA and/or HCV antibodies. Cumulative incidence rates (95% CI) of HCV infection were calculated assuming a Poisson distribution. Cox proportional hazards regression models were fit adjusting for age, sex, race, years of injection drug use, homelessness, and incarceration.
Results: Baseline characteristics of the sample (n = 552) included median age of 23 (interquartile range, 20-26) years; 31.9% female; 73.1% white; 39.7% who did not graduate from high school; and 69.2% who were homeless. During the observation period of 680 person-years, 171 incident cases of HCV infection occurred (incidence rate, 25.1 [95% CI, 21.6-29.2] per 100 person-years). The rate ratio was significantly lower for participants who reported recent maintenance opioid agonist therapy (0.31 [95% CI, 0.14-0.65]; P = .001) but not for those who reported recent non-opioid agonist forms of treatment (0.63 [95% CI, 0.37-1.08]; P = .09) or opioid agonist detoxification (1.45 [95% CI, 0.80-2.69]; P = .23). After adjustment for other covariates, maintenance opioid agonist therapy was associated with lower relative hazards for acquiring HCV infection over time (adjusted hazard ratio, 0.39 [95% CI, 0.18-0.87]; P = .02).
Conclusions and relevance: In this cohort of young adult injection drug users, recent maintenance opioid agonist therapy was associated with a lower incidence of HCV infection. Maintenance treatment with methadone or buprenorphine for opioid use disorders may be an important strategy to prevent the spread of HCV infection among young injection drug users.
Conflict of interest statement
The authors do not have financial conflicts of interest to declare. All authors contributed significantly (see below) and have approved of the manuscript.
Figures
References
-
- Williams IT, Bell BP, Kuhnert W, Alter MJ. Incidence and transmission patterns of acute hepatitis C in the United States, 1982–2006. Arch. Intern. Med. 2011 Feb 14;171(3):242–248. - PubMed
-
- Surveillance for Acute Viral Hepatitis - United States, 2006. MMWR; 2008. Centers for Disease Control and Prevention.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
