

Early prediction of intensive care unit-acquired weakness using easily available parameters: a prospective observational study
- PMID: 25347675
- PMCID: PMC4210178
- DOI: 10.1371/journal.pone.0111259
Early prediction of intensive care unit-acquired weakness using easily available parameters: a prospective observational study
Abstract
Introduction: An early diagnosis of Intensive Care Unit-acquired weakness (ICU-AW) using muscle strength assessment is not possible in most critically ill patients. We hypothesized that development of ICU-AW can be predicted reliably two days after ICU admission, using patient characteristics, early available clinical parameters, laboratory results and use of medication as parameters.
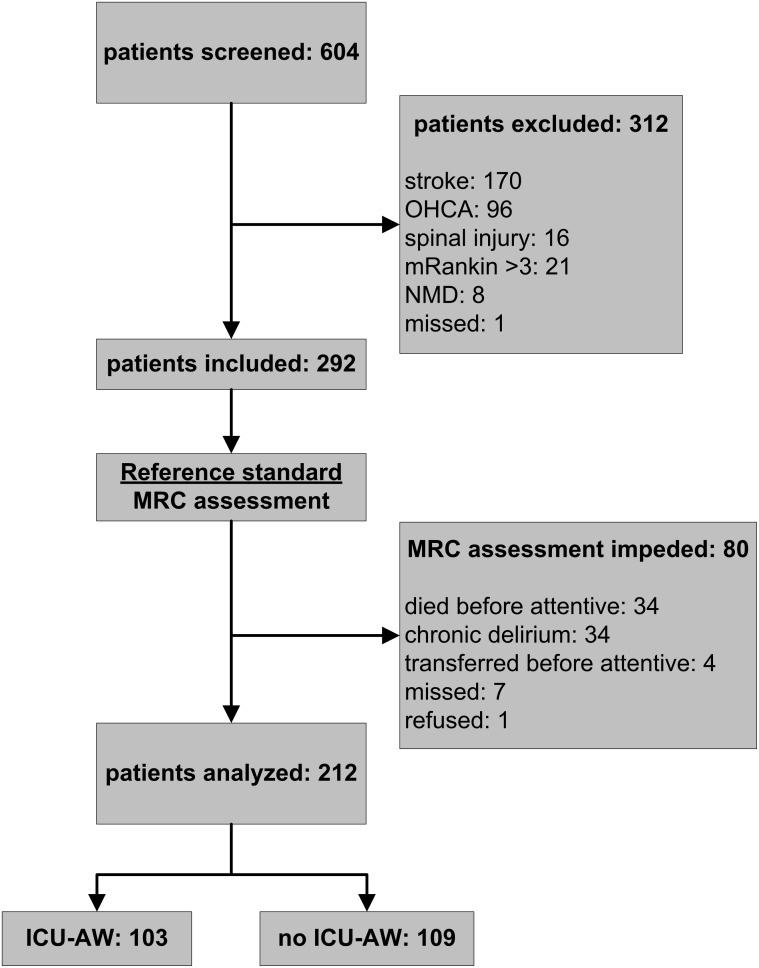
Methods: Newly admitted ICU patients mechanically ventilated ≥2 days were included in this prospective observational cohort study. Manual muscle strength was measured according to the Medical Research Council (MRC) scale, when patients were awake and attentive. ICU-AW was defined as an average MRC score <4. A prediction model was developed by selecting predictors from an a-priori defined set of candidate predictors, based on known risk factors. Discriminative performance of the prediction model was evaluated, validated internally and compared to the APACHE IV and SOFA score.
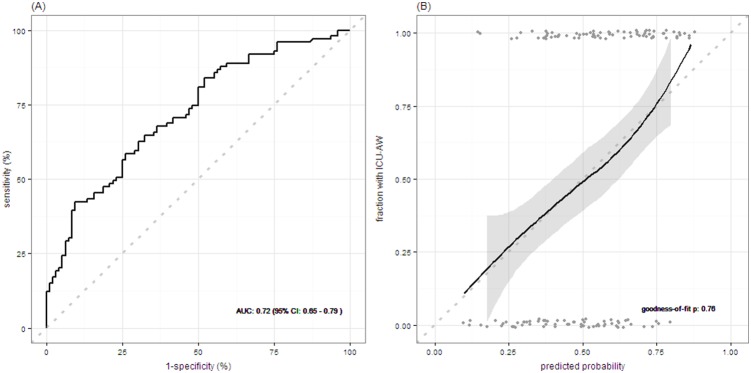
Results: Of 212 included patients, 103 developed ICU-AW. Highest lactate levels, treatment with any aminoglycoside in the first two days after admission and age were selected as predictors. The area under the receiver operating characteristic curve of the prediction model was 0.71 after internal validation. The new prediction model improved discrimination compared to the APACHE IV and the SOFA score.
Conclusion: The new early prediction model for ICU-AW using a set of 3 easily available parameters has fair discriminative performance. This model needs external validation.
Conflict of interest statement
Figures
References
-
- Stevens RD, Marshall SA, Cornblath DR, Hoke A, Needham DM, et al. (2009) A framework for diagnosing and classifying intensive care unit-acquired weakness. Crit Care Med 37: S299–308. - PubMed
-
- Latronico N, Bolton CF (2011) Critical illness polyneuropathy and myopathy: a major cause of muscle weakness and paralysis. Lancet Neurol 10: 931–941. - PubMed
-
- Latronico N, Shehu I, Seghelini E (2005) Neuromuscular sequelae of critical illness. Curr Opin Crit Care 11: 381–390. - PubMed
-
- Ali NA, O’Brien JM, Hoffmann SP, Phillips G, Garland A, et al. (2008) Acquired weakness, handgrip strength, and mortality in critically ill patients. Am J Respir Crit Care Med 178: 261–268. - PubMed
-
- Sharshar T, Bastuji-Garin S, Stevens RD, Durand M-C, Malissin I, et al. (2009) Presence and severity of intensive care unit-acquired paresis at time of awakening are associated with increased intensive care unit and hospital mortality. Crit Care Med 37: 3047–3053. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
