

Direct costs of hypertensive patients admitted to hospital in Vietnam- a bottom-up micro-costing analysis
- PMID: 25348043
- PMCID: PMC4221683
- DOI: 10.1186/s12913-014-0514-4
Direct costs of hypertensive patients admitted to hospital in Vietnam- a bottom-up micro-costing analysis
Abstract
Background: There is an economic burden associated with hypertension both worldwide and in Vietnam. In Vietnam, patients with uncontrolled high blood pressure are hospitalized for further diagnosis and initiation of treatment. Because there is no evidence on costs of inpatient care for hypertensive patients available yet to inform policy makers, health insurance and hospitals, this study aims to quantify direct costs of inpatient care for these patients in Vietnam.
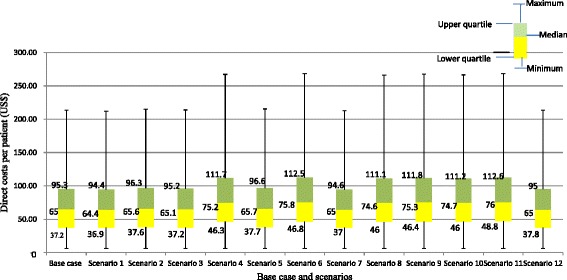
Methods: A retrospective study was conducted in a hospital in Vietnam. Direct costs were analyzed from the health-care provider's perspective. Hospital-based costing was performed using both bottom-up and micro-costing methods. Patients with sole essential or primary hypertension (ICD-code I10) and those comorbid with sphingolipid metabolism or other lipid storage disorders (ICD-code E75) were selected. Costs were quantified based on financial and other records of the hospital. Total cost per patient resulted from an aggregation of laboratory test costs, drug costs, inpatient-days' costs and other remaining costs, including appropriate allocation of overheads. Both mean and medians, as well as interquartile ranges (IQRs) were calculated. In addition to a base-case analysis, specific scenarios were analyzed.
Results: 230 patients were included in the study (147 cases with I10 code only and 83 cases with I10 combined with E75). Median length of hospital stay was 6 days. Median total direct costs per patient were US$65 (IQR: 37 -95). Total costs per patient were higher in the combined hypertensive and lipid population than in the sole hypertensive population at US$78 and US$53, respectively. In all scenarios, hospital inpatient days' costs were identified as the major cost driver in the total costs.
Conclusions: Costs of hospitalization of hypertensive patients is relatively high compared to annual medication treatment at a community health station for hypertension as well as to the total health expenditure per capita in Vietnam. Given that untreated/undetected hypertension likely leads to more expensive treatments of complications, these findings may justify investments by the Vietnamese health-care sector to control high blood pressure in order to save downstream health care budgets.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
