

Prenatal versus postnatal repair procedures for spina bifida for improving infant and maternal outcomes
- PMID: 25348498
- PMCID: PMC6769184
- DOI: 10.1002/14651858.CD008825.pub2
Prenatal versus postnatal repair procedures for spina bifida for improving infant and maternal outcomes
Abstract
Background: Spina bifida is a fetal neural tube defect (NTD), which may be diagnosed in utero and is compatible with life postnatally, albeit often with significant disability and morbidity. Although postnatal repair is possible, with increasing in utero diagnosis with ultrasound, the condition has been treated during pregnancy (prenatal repair) with the aim of decreased morbidity for the child. The procedure that is performed during pregnancy does have potential morbidities for the mother, as it involves maternal surgery to access the fetus.
Objectives: To compare the effects of prenatal versus postnatal repair and different types of repair of spina bifida on perinatal mortality and morbidity, longer term infant outcomes and maternal morbidity.
Search methods: We searched the Cochrane Pregnancy and Childbirth Group's Trials Register (31 July 2014).
Selection criteria: All published, unpublished, and ongoing randomised controlled trials comparing prenatal and postnatal repair of meningomyelocele for fetuses with spina bifida and different types of prenatal repair.
Data collection and analysis: Two review authors independently evaluated trials for inclusion and methodological quality without consideration of their results according to the stated eligibility criteria and extracted data.
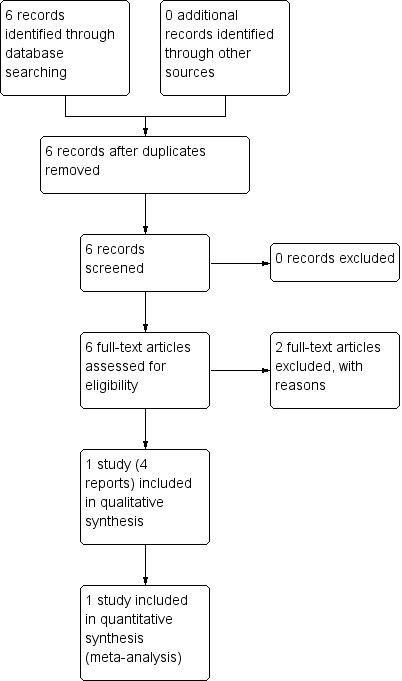
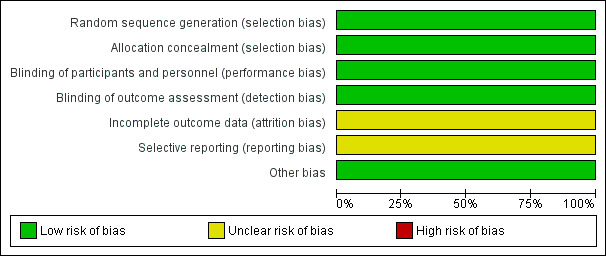
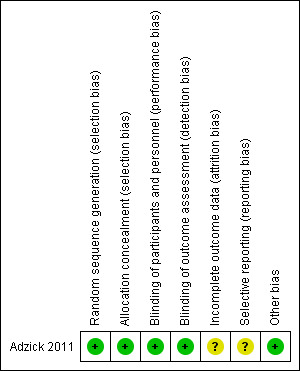
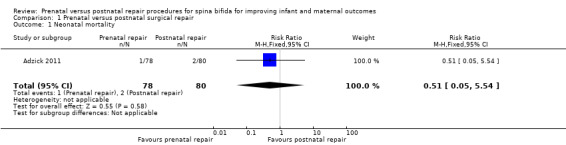
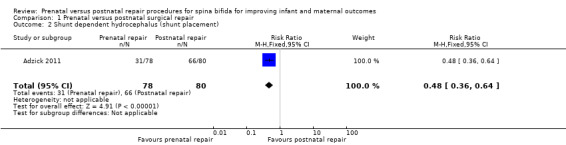
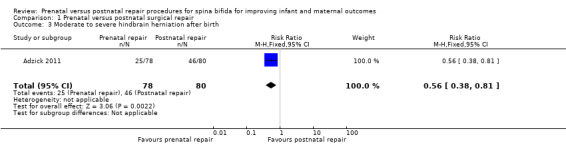
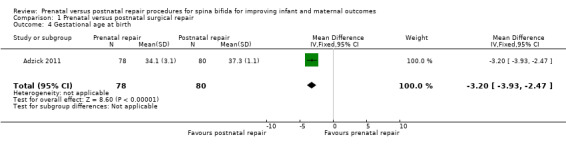
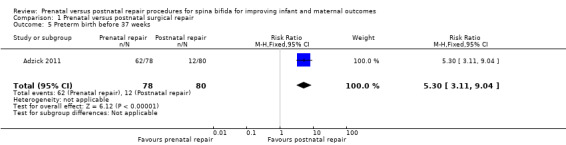
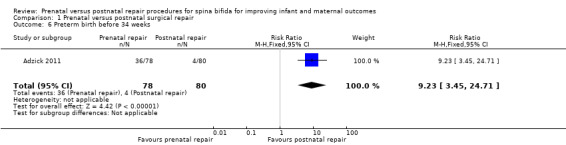
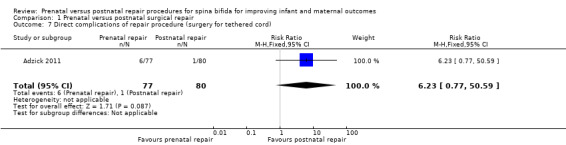
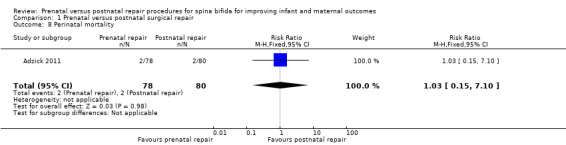
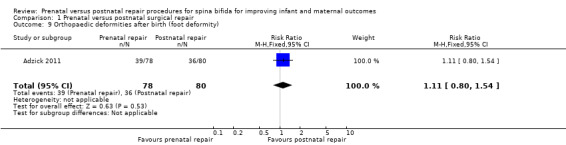
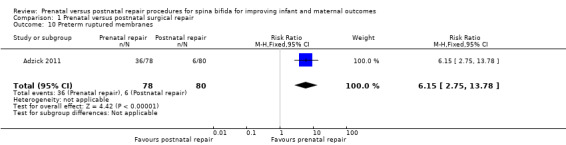
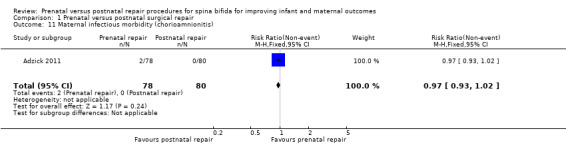
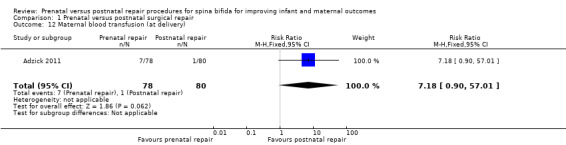
Main results: Our search strategy identified six reports for potential inclusion. Of those, we included one trial (four reports) involving 158 women, which was at low risk of bias.The one included trial examined the effect of prenatal repair versus postnatal repair. For the primary infant outcome of neonatal mortality, there was no clear evidence of a difference identified for prenatal versus postnatal repair (one study, 158 infants, risk ratio (RR) 0.51, 95% confidence interval (CI) 0.05 to 5.54), however event rates were uncommon and so the analysis is likely to be underpowered to detect differences.Prenatal repair was associated with an earlier gestational age at birth (one study, 158 infants, mean difference (MD) -3.20 weeks, 95% CI -3.93 to -2.47) and a corresponding increase in both the risk of preterm birth before 37 weeks (one study, 158 infants, RR 5.30, 95% CI 3.11 to 9.04) and preterm birth before 34 weeks (one study, 158 infants, RR 9.23, 95% CI 3.45 to 24.71). Prenatal repair was associated with a reduction in shunt dependent hydrocephalus and moderate to severe hindbrain herniation. For women, prenatal repair was associated with increased preterm ruptured membranes (one study, 158 women, RR 6.15, 95% CI 2.75 to 13.78), although there was no clear evidence of difference in the risk of chorioamnionitis or blood transfusion, although again, event rates were uncommon.A number of this review's secondary infant and maternal outcomes were not reported. For the infant: days of hospital admission; survival to discharge; stillbirth; need for further surgery (e.g. skin grafting); neurogenic bladder dysfunction; childhood/infant quality of life. For the mother: admission to intensive care; women's emotional wellbeing and satisfaction with care.
Authors' conclusions: This review is based one small well-conducted study. There is insufficient evidence to recommend drawing firm conclusions on the benefits or harms of prenatal repair as an intervention for fetuses with spina bifida. Current evidence is limited by the small number of pregnancies that have been included in the single conducted randomised trial to date.
Conflict of interest statement
None known.
Figures
Update of
- doi: 10.1002/14651858.CD008825
Similar articles
-
Prenatal interventions for congenital diaphragmatic hernia for improving outcomes.Cochrane Database Syst Rev. 2015 Nov 27;2015(11):CD008925. doi: 10.1002/14651858.CD008925.pub2. Cochrane Database Syst Rev. 2015. PMID: 26611822 Free PMC article.
-
Use of biochemical tests of placental function for improving pregnancy outcome.Cochrane Database Syst Rev. 2015 Nov 25;2015(11):CD011202. doi: 10.1002/14651858.CD011202.pub2. Cochrane Database Syst Rev. 2015. PMID: 26602956 Free PMC article.
-
Immediate versus deferred delivery of the preterm baby with suspected fetal compromise for improving outcomes.Cochrane Database Syst Rev. 2016 Jul 12;7(7):CD008968. doi: 10.1002/14651858.CD008968.pub3. Cochrane Database Syst Rev. 2016. PMID: 27404120 Free PMC article.
-
Incentives for increasing prenatal care use by women in order to improve maternal and neonatal outcomes.Cochrane Database Syst Rev. 2015 Dec 15;2015(12):CD009916. doi: 10.1002/14651858.CD009916.pub2. Cochrane Database Syst Rev. 2015. PMID: 26671418 Free PMC article.
-
Planned early delivery versus expectant management of the term suspected compromised baby for improving outcomes.Cochrane Database Syst Rev. 2015 Nov 24;2015(11):CD009433. doi: 10.1002/14651858.CD009433.pub2. Cochrane Database Syst Rev. 2015. PMID: 26599471 Free PMC article.
Cited by
-
Interventions during pregnancy to prevent preterm birth: an overview of Cochrane systematic reviews.Cochrane Database Syst Rev. 2018 Nov 14;11(11):CD012505. doi: 10.1002/14651858.CD012505.pub2. Cochrane Database Syst Rev. 2018. PMID: 30480756 Free PMC article.
-
Neuropathic bladders: Investigation and treatment through their lifetime.Can Urol Assoc J. 2017 Jan-Feb;11(1-2Suppl1):S81-S86. doi: 10.5489/cuaj.4276. Can Urol Assoc J. 2017. PMID: 28265327 Free PMC article. Review.
-
Placenta as a source of autologous graft in postnatal correction of myelomeningocele.Childs Nerv Syst. 2024 Dec;40(12):4115-4121. doi: 10.1007/s00381-024-06635-x. Epub 2024 Sep 30. Childs Nerv Syst. 2024. PMID: 39343858
-
Practice-changing publications: Pediatric urology - focus on treatment of spina bifida.Can Urol Assoc J. 2021 Oct;15(10):324-325. doi: 10.5489/cuaj.7590. Can Urol Assoc J. 2021. PMID: 34665123 Free PMC article. No abstract available.
-
A Single-Centre Analysis of Surgical Techniques for Myelomeningocele Closure: Methods, Outcomes, and Complications.Clin Pract. 2024 Sep 29;14(5):2056-2070. doi: 10.3390/clinpract14050162. Clin Pract. 2024. PMID: 39451877 Free PMC article.
References
References to studies included in this review
Adzick 2011 {published data only}
-
- Anonymous. MOMS management of myelomeningocele study. http://www.spinabifidamoms.com/english/overview.html (accessed 22 July 2003).
-
- Spong C. Myelomeningocele repair randomized trial. http://clinicaltrials.gov/ct2/show/NCT00060606 (accessed 18 March 2011) 2011.
-
- Thom E, Burrows PK, Adzick S, Yang E, Spong C. Management of myelomeningocele study: status after five years. Prenatal Diagnosis 2008;28:S23.
References to studies excluded from this review
Almodin 2006 {published data only}
-
- Almodin CG, Moron AF, Cavaliero S, Yamashita A, Hisaba W, Piassi J. The Almodin‐Moron trocar for uterine entry during fetal surgery. Fetal Diagnosis and Therapy 2006;21(5):414‐7. - PubMed
Bruner 1999a {published data only}
-
- Bruner JP, Boehm FH, Tulipan N. The tulipan‐bruner trocar for uterine entry during fetal surgery. American Journal of Obstetrics and Gynecology 1999;181(5 Pt 1):1188‐91. - PubMed
Additional references
Adzick 1998
-
- Adzick NS, Sutton LN, Crombleholme TM, Flake AW. Successful fetal surgery for spina bifida. Lancet 1998;352:1675‐6. - PubMed
AIHW 2004
-
- AIHW National Perinatal Statistics Unit. Australia's babies: their health and wellbeing. Bulletin no. 21. AIHW cat. no. AUS 54. Canberra: AIHW NPSU, 2004.
Bruner 1999
-
- Bruner JP, Richards WO, Tulipan NB, Arney TL. Endoscopic coverage of fetal myelomeningocele in utero. Americal Journal of Obstetrics and Gynecology 1999;180(1 Pt 1):153‐8. - PubMed
Higgins 2011
-
- Higgins JPT, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Mitchell 2004
-
- Mitchell LE, Adzick NS, Melchionne J, Pasquariello PS, Sutton LN, Whitehead AS. Spina bifida. Lancet 2004;364(9448):1885‐95. - PubMed
RevMan 2014 [Computer program]
-
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Sutton 2008
Tulipan 1998
-
- Tulipan N, Bruner JP. Myelomeningocele repair in utero: a report of three cases. Pediatric Neurosurgery 1998;28(4):177‐80. - PubMed
Tulipan 1999
-
- Tulipan N, Bruner JP, Hernanz‐Schulman M, Lowe LH, Walsh WF, Nickolaus D, et al. Effect of intrauterine myelomeningocele repair on central nervous system structure and function. Pediatric Neurosurgery 1999;31:183‐8. - PubMed
Tulipan 2003
-
- Tulipan N, Sutton LN, Bruner JP, Cohen BM, Johnson M, Adzick NS. The effect of intrauterine myelomeningocele repair on the incidence of shunt dependent hydrocephalus. Pediatric Neurosurgery 2003;38(1):27‐33. - PubMed
Walsh 2003
-
- Walsh DS, Adzick NS. Foetal surgery for spina bifida. Seminars in Neonatology 2003;8:197‐205. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical