

Rapamycin ameliorates IgA nephropathy via cell cycle-dependent mechanisms
- PMID: 25349217
- PMCID: PMC4935411
- DOI: 10.1177/1535370214555666
Rapamycin ameliorates IgA nephropathy via cell cycle-dependent mechanisms
Abstract
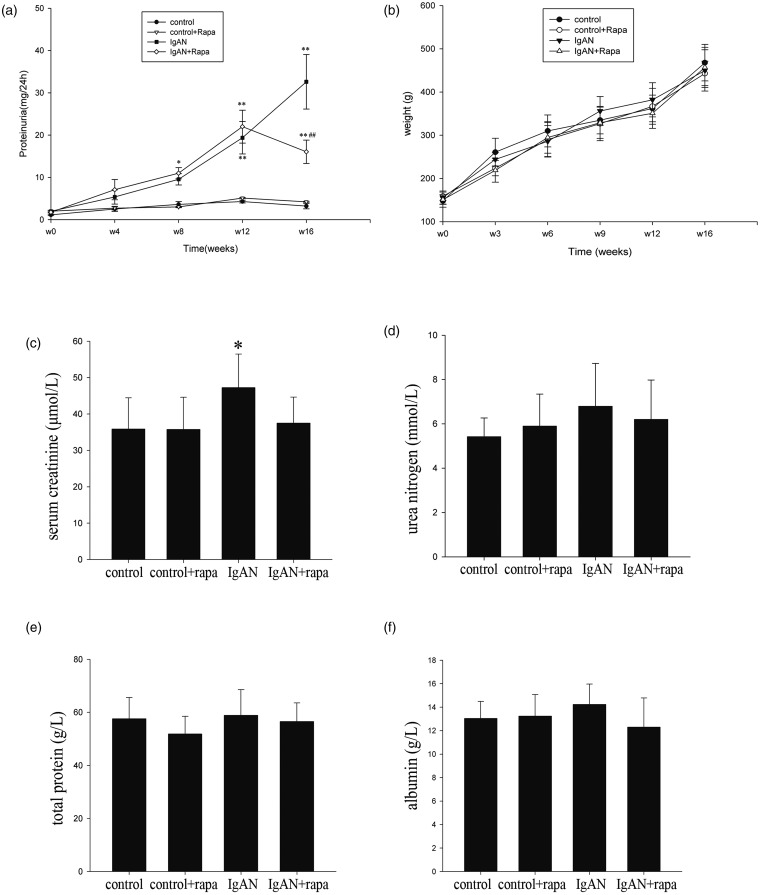
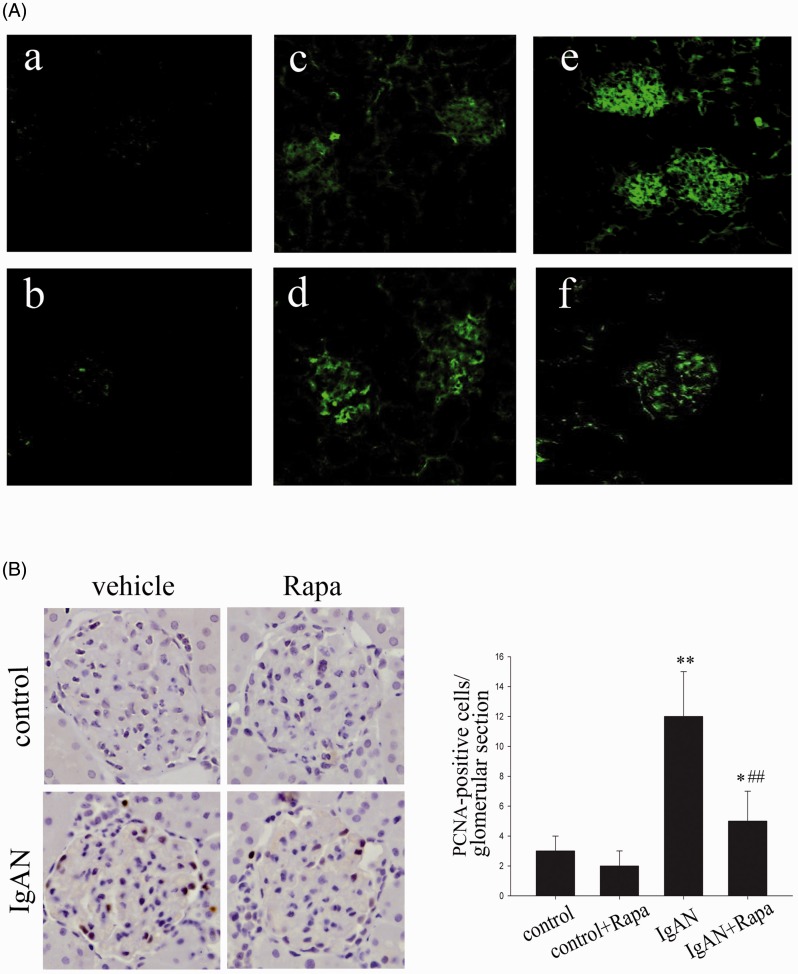
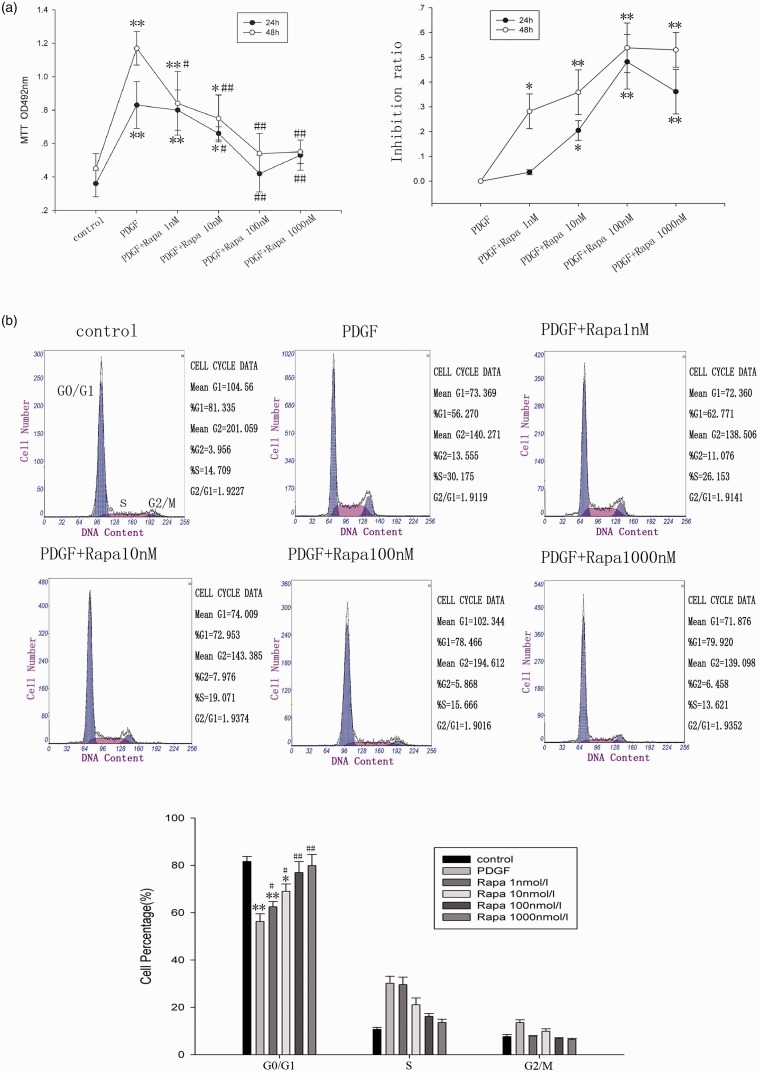
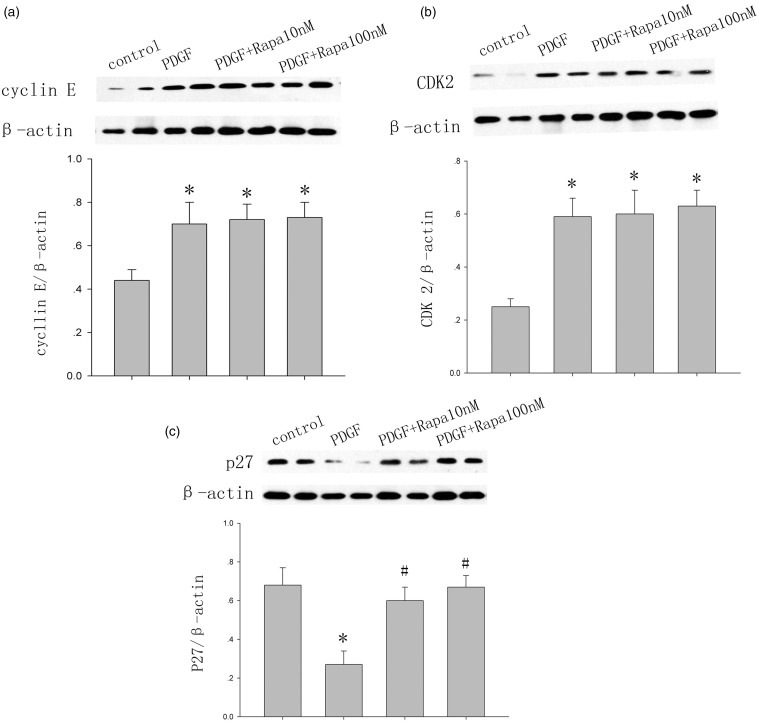
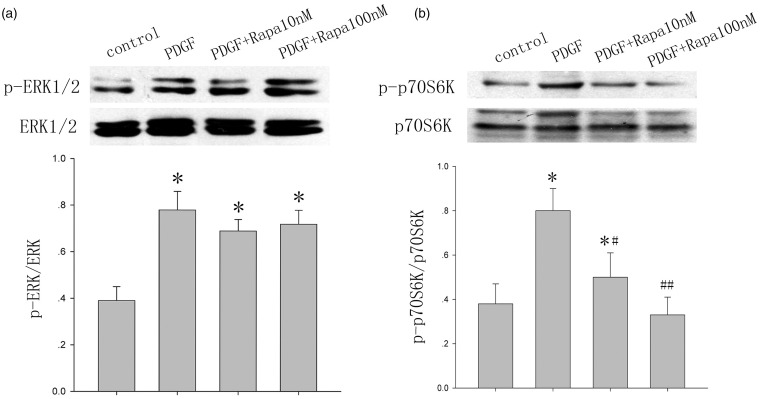
IgA nephropathy is the most frequent type of glomerulonephritis worldwide. The role of cell cycle regulation in the pathogenesis of IgA nephropathy has been studied. The present study was designed to explore whether rapamycin ameliorates IgA nephropathy via cell cycle-dependent mechanisms. After establishing an IgA nephropathy model, rats were randomly divided into four groups. Coomassie Brilliant Blue was used to measure the 24-h urinary protein levels. Renal function was determined using an autoanalyzer. Proliferation was assayed via Proliferating Cell Nuclear Antigen (PCNA) immunohistochemistry. Rat mesangial cells were cultured and divided into the six groups. Methylthiazolyldiphenyl-tetrazolium bromide (MTT) and flow cytometry were used to detect cell proliferation and the cell cycle phase. Western blotting was performed to determine cyclin E, cyclin-dependent kinase 2, p27(Kip1), p70S6K/p-p70S6K, and extracellular signal-regulated kinase 1/2/p- extracellular signal-regulated kinase 1/2 protein expression. A low dose of the mammalian target of rapamycin (mTOR) inhibitor rapamycin prevented an additional increase in proteinuria, protected kidney function, and reduced IgA deposition in a model of IgA nephropathy. Rapamycin inhibited mesangial cell proliferation and arrested the cell cycle in the G1 phase. Rapamycin did not affect the expression of cyclin E and cyclin-dependent kinase 2. However, rapamycin upregulated p27(Kip1) at least in part via AKT (also known as protein kinase B)/mTOR. In conclusion, rapamycin can affect cell cycle regulation to inhibit mesangial cell proliferation, thereby reduce IgA deposition, and slow the progression of IgAN.
Keywords: IgA nephropathy; Rapamycin; cell cycle proteins; mesangial cell.
© 2014 by the Society for Experimental Biology and Medicine.
Figures
References
-
- Donadio JV, Grande JP. IgA nephropathy. N Engl J Med 2002; 347(10): 738–48. - PubMed
-
- Floege J, Feehally J. IgA nephropathy: recent developments. J Am Soc Nephrol 2000; 11(12): 2395–403. - PubMed
-
- Lai KN. Pathogenesis of IgA nephropathy. Nat Rev Nephrol 2012; 8(5): 275–283. - PubMed
-
- Kurogi Y. Mesangial cell proliferation inhibitors for the treatment of proliferative glomerular disease. Med Res Rev 2003; 23(1): 15–31. - PubMed
-
- Shankland SJ. Cell cycle regulatory proteins in glomerular disease. Kidney Int 1999; 56(4): 1208–15. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous