

Skeletal dysplasias: A radiographic approach and review of common non-lethal skeletal dysplasias
- PMID: 25349664
- PMCID: PMC4209426
- DOI: 10.4329/wjr.v6.i10.808
Skeletal dysplasias: A radiographic approach and review of common non-lethal skeletal dysplasias
Abstract
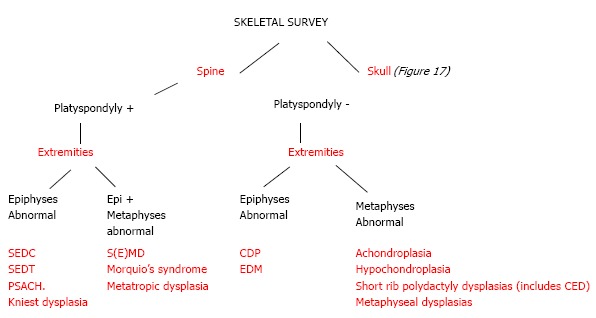
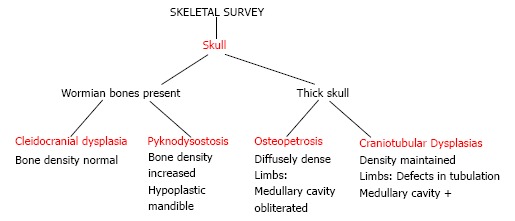
Skeletal dysplasias are not uncommon entities and a radiologist is likely to encounter a suspected case of dysplasia in his practice. The correct and early diagnosis of dysplasia is important for management of complications and for future genetic counselling. While there is an exhaustive classification system on dysplasias, it is important to be familiar with the radiological features of common dysplasias. In this article, we enumerate a radiographic approach to skeletal dysplasias, describe the essential as well as differentiating features of common non-lethal skeletal dysplasias and conclude by presenting working algorithms to either definitively diagnose a particular dysplasia or suggest the most likely differential diagnoses to the referring clinician and thus direct further workup of the patient.
Keywords: Achondroplasia; Algorithm; Approach; Multiple epiphyseal dysplasia; Radiograph; Review; Rhizomelia; Short limb dwarfism; Skeletal dysplasia; Skeletal survey; Spondylopepiphyseal dysplasia.
Figures







References
-
- Offiah AC, Hall CM. Radiological diagnosis of the constitutional disorders of bone. As easy as A, B, C? Pediatr Radiol. 2003;33:153–161. - PubMed
-
- Barbosa-Buck CO, Orioli IM, da Graça Dutra M, Lopez-Camelo J, Castilla EE, Cavalcanti DP. Clinical epidemiology of skeletal dysplasias in South America. Am J Med Genet A. 2012;158A:1038–1045. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
