

Delayed cerebral radiation necrosis after neutron beam radiation of a parotid adenocarcinoma: a case report and review of the literature
- PMID: 25349750
- PMCID: PMC4198779
- DOI: 10.1155/2014/717984
Delayed cerebral radiation necrosis after neutron beam radiation of a parotid adenocarcinoma: a case report and review of the literature
Abstract
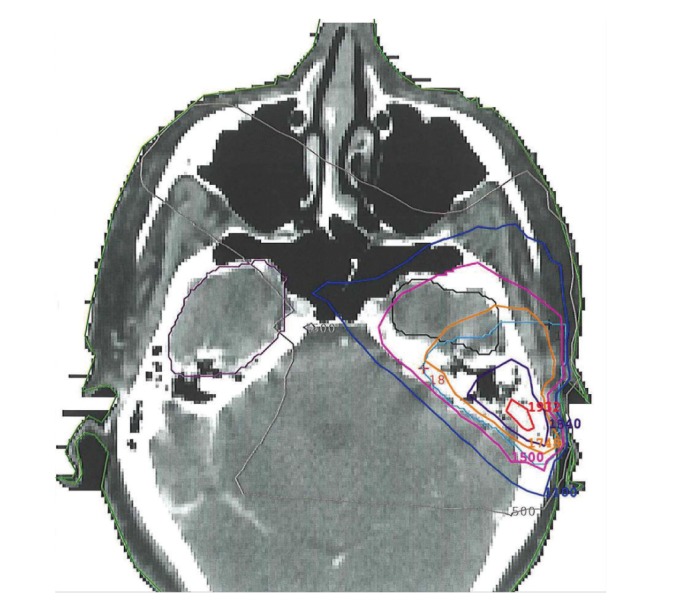
Cerebral radiation necrosis (CRN) is a well described possible complication of radiation for treatment of intracranial pathology. However, CRN as sequelae of radiation to extracranial sites is rare. Neutron beam radiation is a highly potent form of radiotherapy that may be used to treat malignant tumors of the salivary glands. This report describes a patient who underwent neutron beam radiation for a parotid adenocarcinoma and who developed biopsy-confirmed temporal lobe radiation necrosis thirty months later. This represents the longest time interval described to date, from initial neutron radiation for extracranial pathology to development of CRN. Two other detailed case studies exist in the literature and are described in this report. These reports as well as our patient's case are reviewed, and additional recommendations are made to minimize the development of CRN after extracranial neutron beam radiation. Physicians should include the possible diagnosis of CRN in any patient with new neurologic signs or symptoms and a history of head and neck radiation that included planned fields extending to the base of the skull. Counseling of patients prior to neutron beam radiation should include potential neurologic complications associated with CRN and risks of treatment for CRN including neurosurgical intervention.
Figures



Similar articles
-
Results of excision of cerebral radionecrosis: experience in patients treated with radiation therapy for nasopharyngeal carcinoma.J Neurosurg. 2010 Aug;113(2):293-300. doi: 10.3171/2010.1.JNS091039. J Neurosurg. 2010. PMID: 20151776
-
Characterization of cerebral radiation necrosis following the treatment of sinonasal malignancies.Laryngoscope Investig Otolaryngol. 2024 Mar 23;9(2):e1200. doi: 10.1002/lio2.1200. eCollection 2024 Apr. Laryngoscope Investig Otolaryngol. 2024. PMID: 38525116 Free PMC article.
-
The safety of magnetic resonance imaging-guided laser interstitial thermal therapy for cerebral radiation necrosis.J Neurooncol. 2018 Jul;138(3):609-617. doi: 10.1007/s11060-018-2828-2. Epub 2018 Mar 13. J Neurooncol. 2018. PMID: 29536345
-
Delayed radiation necrosis of brainstem related to fast neutron beam irradiation: case report and literature review.Cancer. 1979 Aug;44(2):473-9. doi: 10.1002/1097-0142(197908)44:2<473::aid-cncr2820440215>3.0.co;2-5. Cancer. 1979. PMID: 224999 Review.
-
Temporal Lobe Necrosis Following Radiotherapy in Nasopharyngeal Carcinoma: New Insight Into the Management.Front Oncol. 2021 Jan 21;10:593487. doi: 10.3389/fonc.2020.593487. eCollection 2020. Front Oncol. 2021. PMID: 33552967 Free PMC article. Review.
Cited by
-
Late post-treatment radiographic changes 3 years following chemoradiation for glioma: the importance of histopathology.CNS Oncol. 2017 Jul 18;6(3):195-201. doi: 10.2217/cns-2016-0040. Online ahead of print. CNS Oncol. 2017. PMID: 28718307 Free PMC article.
-
Radiation-induced temporal lobe necrosis in a nasopharyngeal cancer patient after external beam radiotherapy: a case report and review of literature.J Med Case Rep. 2025 Jul 12;19(1):339. doi: 10.1186/s13256-025-05368-y. J Med Case Rep. 2025. PMID: 40652209 Free PMC article. Review.
References
-
- Cross NE, Glantz MJ. Neurologic complications of radiation therapy. Neurologic Clinics. 2003;21(1):249–277. - PubMed
-
- Delanian S, Lefaix JL. Reversing the radiation-induced fibro-atrophic process. La Revue de Médecine Interne. 2002;23(2):164–174. - PubMed
-
- Wang XF, Zhang S, Ye YH, Chen YP, Liu XY. Clinicopathologic features of delayed radiation-induced brain injury after radiotherapy for brain tumor. Chinese Journal of Pathology. 2012;41:224–228. - PubMed
-
- Emami B, Lyman J, Brown A, et al. Tolerance of normal tissue to therapeutic irradiation. International Journal of Radiation Oncology Biology Physics. 1991;21(1):109–122. - PubMed
-
- Blonigen BJ, Steinmetz RD, Levin L, Lamba MA, Warnick RE, Breneman JC. Irradiated volume as a predictor of brain radionecrosis after linear accelerator stereotactic radiosurgery. International Journal of Radiation Oncology, Biology, Physics. 2010;77(4):996–1001. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
