

Sex-specific differences in hemodialysis prevalence and practices and the male-to-female mortality rate: the Dialysis Outcomes and Practice Patterns Study (DOPPS)
- PMID: 25350533
- PMCID: PMC4211675
- DOI: 10.1371/journal.pmed.1001750
Sex-specific differences in hemodialysis prevalence and practices and the male-to-female mortality rate: the Dialysis Outcomes and Practice Patterns Study (DOPPS)
Abstract
Background: A comprehensive analysis of sex-specific differences in the characteristics, treatment, and outcomes of individuals with end-stage renal disease undergoing dialysis might reveal treatment inequalities and targets to improve sex-specific patient care. Here we describe hemodialysis prevalence and patient characteristics by sex, compare the adult male-to-female mortality rate with data from the general population, and evaluate sex interactions with mortality.
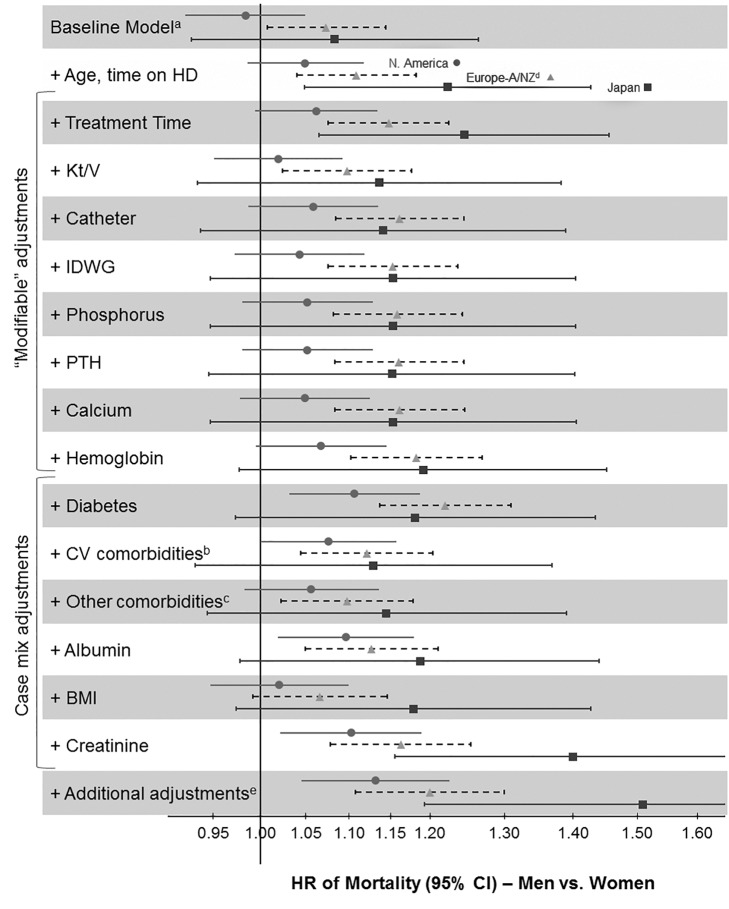
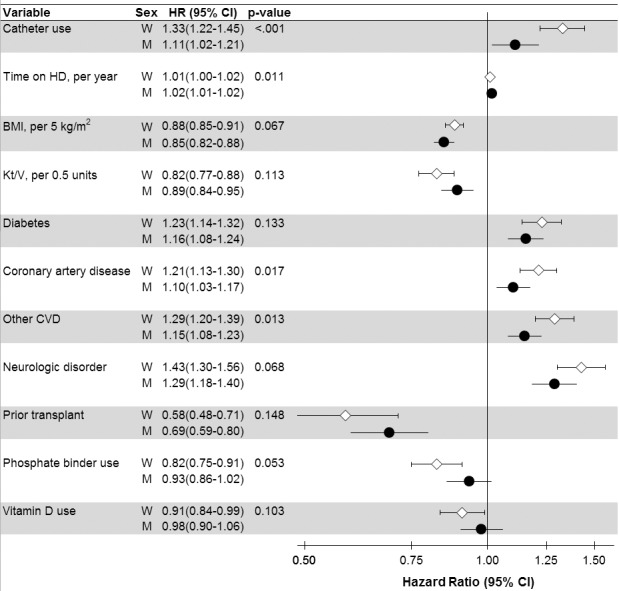
Methods and findings: We assessed the Human Mortality Database and 206,374 patients receiving hemodialysis from 12 countries (Australia, Belgium, Canada, France, Germany, Italy, Japan, New Zealand, Spain, Sweden, the UK, and the US) participating in the international, prospective Dialysis Outcomes and Practice Patterns Study (DOPPS) between June 1996 and March 2012. Among 35,964 sampled DOPPS patients with full data collection, we studied patient characteristics (descriptively) and mortality (via Cox regression) by sex. In all age groups, more men than women were on hemodialysis (59% versus 41% overall), with large differences observed between countries. The average estimated glomerular filtration rate at hemodialysis initiation was higher in men than women. The male-to-female mortality rate ratio in the general population varied from 1.5 to 2.6 for age groups <75 y, but in hemodialysis patients was close to one. Compared to women, men were younger (mean = 61.9 ± standard deviation 14.6 versus 63.1 ± 14.5 y), were less frequently obese, were more frequently married and recipients of a kidney transplant, more frequently had coronary artery disease, and were less frequently depressed. Interaction analyses showed that the mortality risk associated with several comorbidities and hemodialysis catheter use was lower for men (hazard ratio [HR] = 1.11) than women (HR = 1.33, interaction p<0.001). This study is limited by its inability to establish causality for the observed sex-specific differences and does not provide information about patients not treated with dialysis or dying prior to a planned start of dialysis.
Conclusions: Women's survival advantage was markedly diminished in hemodialysis patients. The finding that fewer women than men were being treated with dialysis for end-stage renal disease merits detailed further study, as the large discrepancies in sex-specific hemodialysis prevalence by country and age group are likely explained by factors beyond biology. Modifiable variables, such as catheter use, showing significant sex interactions suggest interventional targeting. Please see later in the article for the Editors' Summary.
Conflict of interest statement
BMR has received a speaker's fee from Kyowa Hakko Kirin. RLP has received speaker's fees from Amgen, Kyowa Hakko Kirin, and Vifor and has served on an advisory panel for Merck. The other authors have declared that no competing interests exist.
Figures


References
-
- Putting gender on the agenda. Nature 465: 665 doi:10.1038/465665a - DOI - PubMed
-
- Arnold K (2000) Journal to encourage analysis by sex/ethnicity. J Natl Cancer Inst 92: 1561. - PubMed
-
- Taking sex into account in medicine. Lancet 378: 1826 doi:10.1016/S0140-6736(11)61795-9 - DOI - PubMed
-
- Haslam DW, James WP (2005) Obesity. Lancet 366: 1197–1209. - PubMed
-
- Meisinger C, Thorand B, Schneider A, Stieber J, Doring A, et al. (2002) Sex differences in risk factors for incident type 2 diabetes mellitus: the MONICA Augsburg cohort study. Arch Intern Med 162: 82–89. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
