

Readmission rates and long-term hospital costs among survivors of an in-hospital cardiac arrest
- PMID: 25351479
- PMCID: PMC4241155
- DOI: 10.1161/CIRCOUTCOMES.114.000925
Readmission rates and long-term hospital costs among survivors of an in-hospital cardiac arrest
Abstract
Background: Although an in-hospital cardiac arrest is common, little is known about readmission patterns and an inpatient resource use among survivors of an in-hospital cardiac arrest.
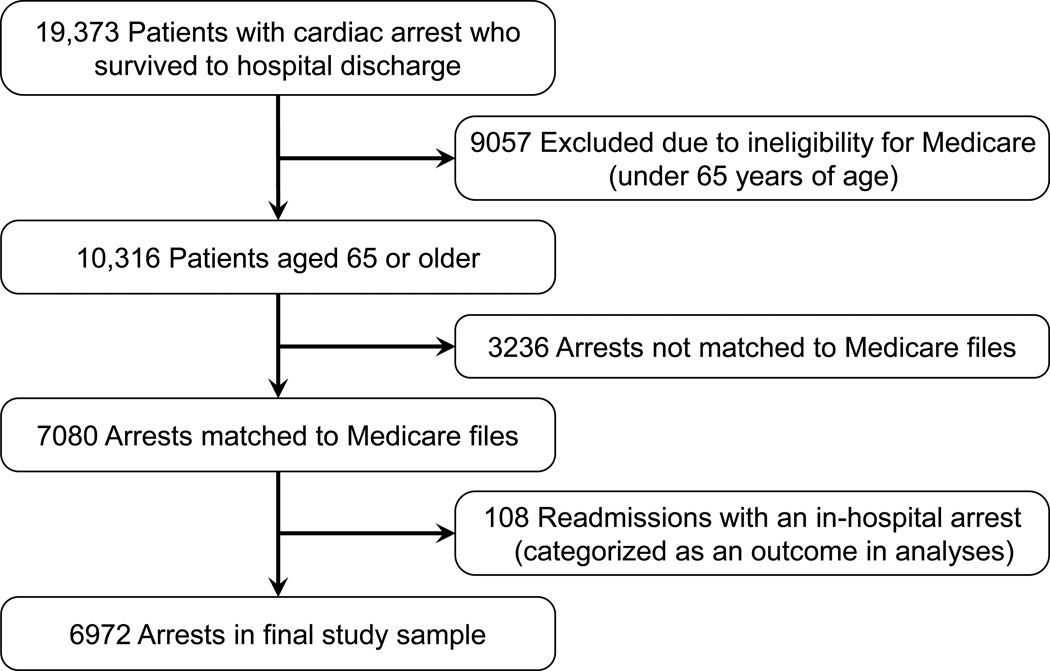
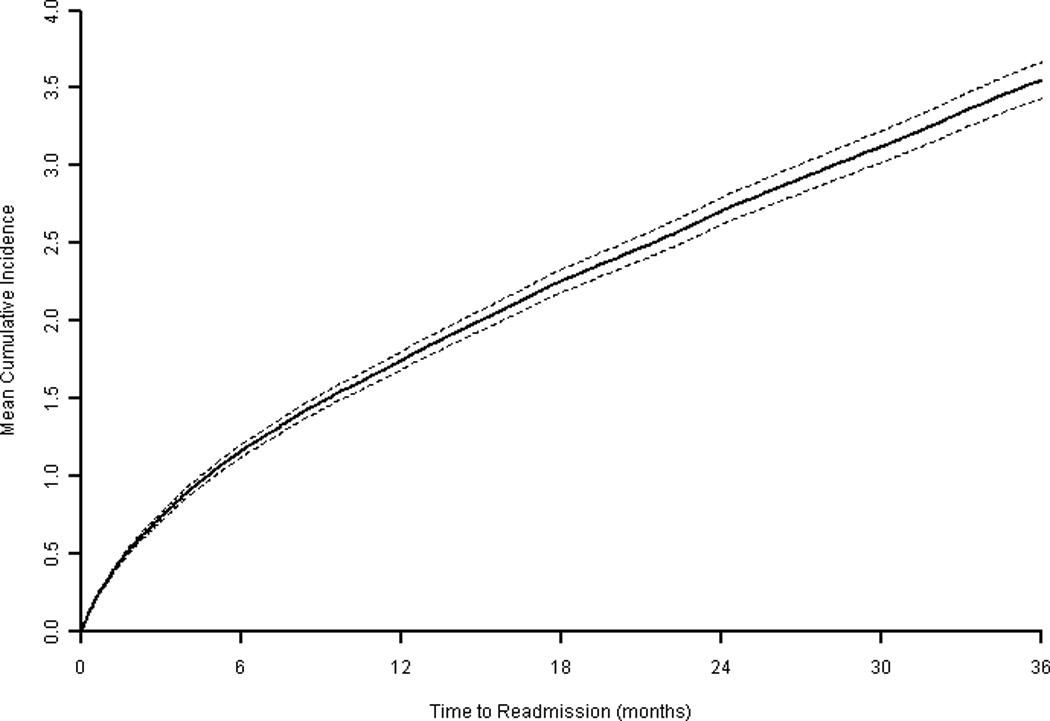
Methods and results: Within a large national registry, we examined long-term inpatient use among 6972 adults aged ≥65 years who survived an in-hospital cardiac arrest. We examined 30-day and 1-year readmission rates and inpatient costs, overall and by patient demographics, hospital disposition (discharge destination), and neurological status at discharge. The mean age was 75.8±7.0 years, 56% were men, and 12% were black. There were a total of 2005 readmissions during the first 30 days (cumulative incidence rate, 35 readmissions/100 patients; 95% confidence interval, 33-37) and 8751 readmissions at 1 year (cumulative incidence rate, 185 readmissions/100 patients; 95% confidence interval, 177-190). Overall, mean inpatient costs were $7741±$2323 at 30 days and $18 629±$9411 at 1 year. Thirty-day inpatient costs were higher in patients of younger age (≥85 years, $6052 [reference]; 75-84 years, $7444 [adjusted cost ratio, 1.23; 1.06-1.42; 65-74 years, $8291 [adjusted cost ratio, 1.37; 1.19-1.59; both P<0.001) and black race (whites, $7413; blacks, $9044; adjusted cost ratio, 1.22; 1.05-1.42; P<0.001), as well as those discharged with severe neurological disability or to skilled nursing or rehabilitation facilities. These differences in resource use persisted at 1 year and were largely because of higher readmission rates.
Conclusions: Survivors of an in-hospital cardiac arrest have frequent readmissions and high follow-up inpatient costs. Readmissions and inpatient costs were higher in certain subgroups, including patients of younger age and black race.
Keywords: costs and cost analysis; heart arrest; outcome assessment (health care); patient readmission.
© 2014 American Heart Association, Inc.
Conflict of interest statement
Dr. Chan has served as a consultant for the American Heart Association. Dr. Krumholz discloses that he is the recipient of a research grant from Medtronic, through Yale University, and is chair of a cardiac scientific advisory board for United Health. None of the other authors has any conflicts of interest or financial interests to disclose.
Figures
References
-
- Peberdy MA, Kaye W, Ornato JP, Larkin GL, Nadkarni V, Mancini ME, Berg RA, Nichol G, Lane-Trultt T. Cardiopulmonary resuscitation of adults in the hospital: a report of 14720 cardiac arrests from the National Registry of Cardiopulmonary Resuscitation. Resuscitation. 2003;58:297–308. - PubMed
-
- Cummins RO, Chamberlain D, Hazinski MF, Nadkarni V, Kloeck W, Kramer E, Becker L, Robertson C, Koster R, Zaritsky A, Bossaert L, Ornato JP, Callanan V, Allen M, Steen P, Connolly B, Sanders A, Idris A, Cobbe S. Recommended guidelines for reviewing, reporting, conducting research on in-hospital resuscitation: the in-hospital ‘Utstein style’. American Heart Association. Circulation. 1997;95:2213–2239. - PubMed
-
- Jacobs I, Nadkarni V, Bahr J, Berg RA, Billi JE, Bossaert L, Cassan P, Coovadia A, D’Este K, Finn J, Halperin H, Handley A, Herlitz J, Hickey R, Idris A, Kloeck W, Larkin GL, Mancini ME, Mason P, Mears G, Monsieurs K, Montgomery W, Morley P, Nichol G, Nolan J, Okada K, Perlman J, Shuster M, Steen PA, Sterz F, Tibballs J, Timerman S, Truitt T, Zideman D. Cardiac arrest and cardiopulmonary resuscitation outcome reports: update and simplification of the Utstein templates for resuscitation registries: a statement for healthcare professionals from a task force of the International Liaison Committee on Resuscitation (American Heart Association, European Resuscitation Council, Australian Resuscitation Council, New Zealand Resuscitation Council, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Councils of Southern Africa) Circulation. 2004;110:3385–3397. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
