

Novel genotype-phenotype associations demonstrated by high-throughput sequencing in patients with hypertrophic cardiomyopathy
- PMID: 25351510
- PMCID: PMC4345808
- DOI: 10.1136/heartjnl-2014-306387
Novel genotype-phenotype associations demonstrated by high-throughput sequencing in patients with hypertrophic cardiomyopathy
Abstract
Objective: A predictable relation between genotype and disease expression is needed in order to use genetic testing for clinical decision-making in hypertrophic cardiomyopathy (HCM). The primary aims of this study were to examine the phenotypes associated with sarcomere protein (SP) gene mutations and test the hypothesis that variation in non-sarcomere genes modifies the phenotype.
Methods: Unrelated and consecutive patients were clinically evaluated and prospectively followed in a specialist clinic. High-throughput sequencing was used to analyse 41 genes implicated in inherited cardiac conditions. Variants in SP and non-SP genes were tested for associations with phenotype and survival.
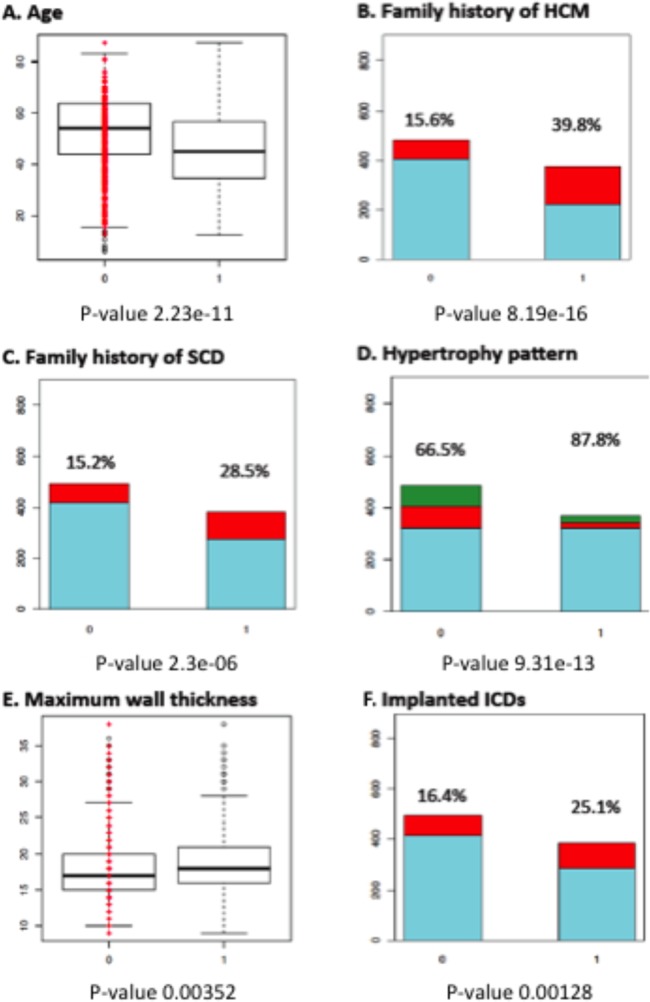
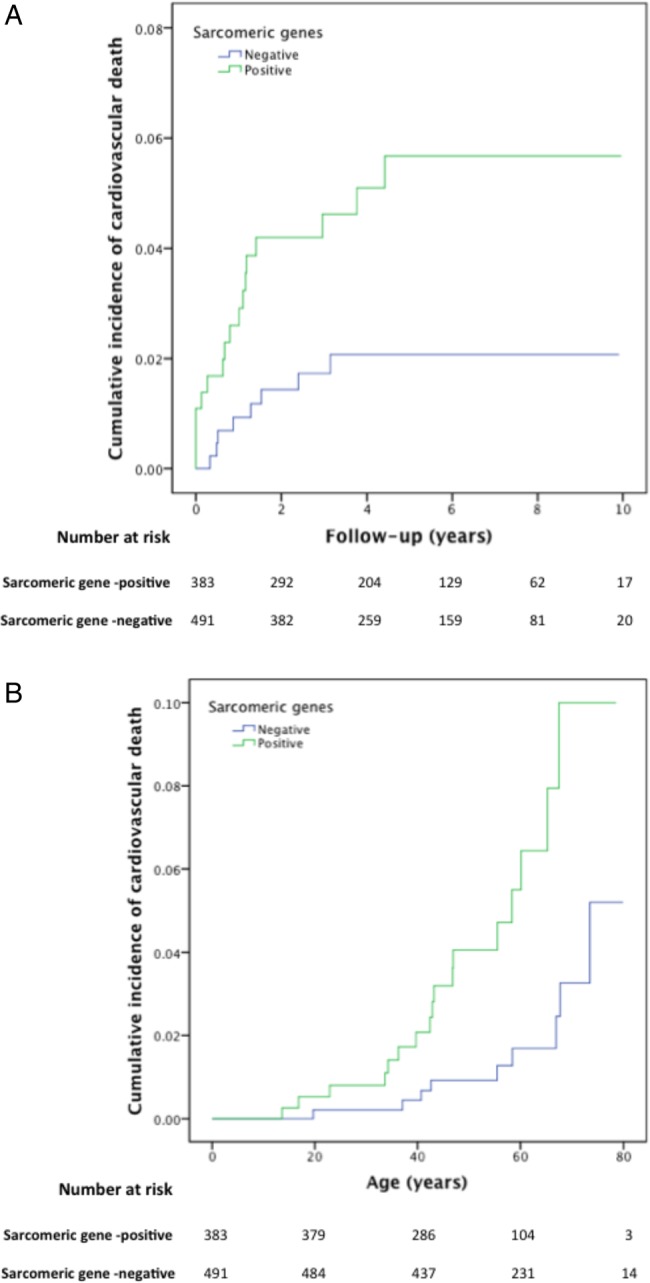
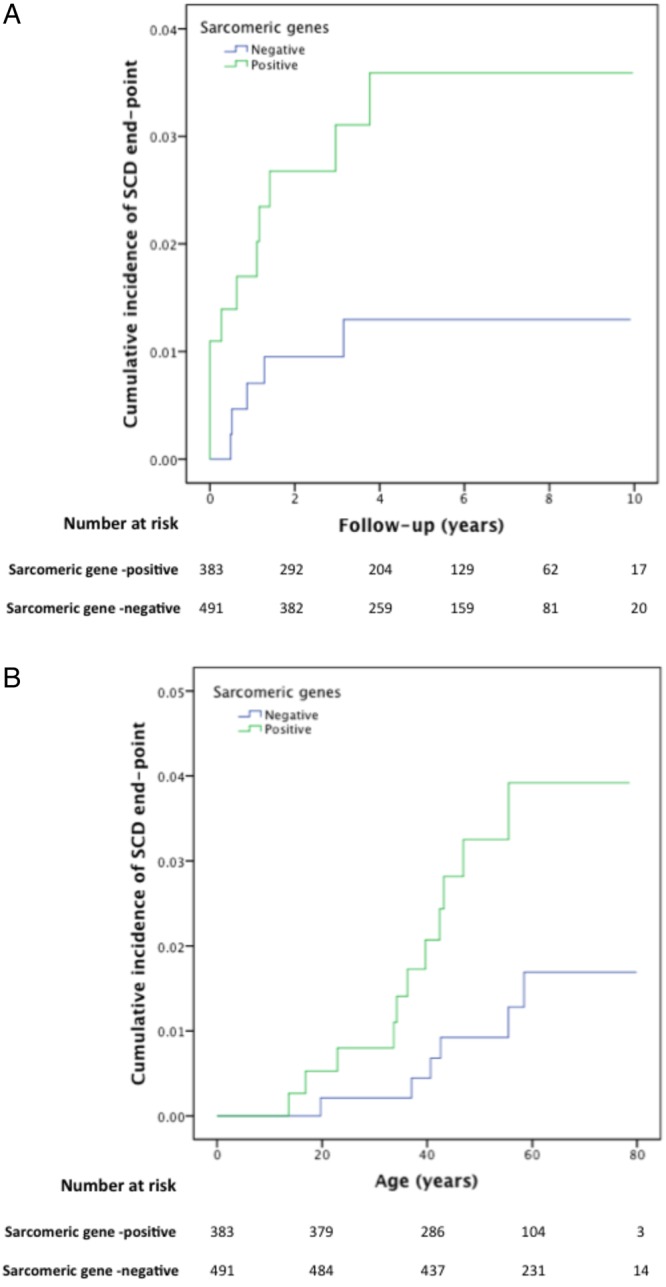
Results: 874 patients (49.6±15.4 years, 67.8% men) were studied; likely disease-causing SP gene variants were detected in 383 (43.8%). Patients with SP variants were characterised by younger age and higher prevalence of family history of HCM, family history of sudden cardiac death, asymmetric septal hypertrophy, greater maximum LV wall thickness (all p values<0.0005) and an increased incidence of cardiovascular death (p=0.012). Similar associations were observed for individual SP genes. Patients with ANK2 variants had greater maximum wall thickness (p=0.0005). Associations at a lower level of significance were demonstrated with variation in other non-SP genes.
Conclusions: Patients with HCM caused by rare SP variants differ with respect to age at presentation, family history of the disease, morphology and survival from patients without SP variants. Novel associations for SP genes are reported and, for the first time, we demonstrate possible influence of variation in non-SP genes associated with other forms of cardiomyopathy and arrhythmia syndromes on the clinical phenotype of HCM.
Keywords: GENETICS.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Figures
References
-
- Elliott P, McKenna WJ. Hypertrophic cardiomyopathy. Lancet 2004; 363:1881–91. - PubMed
-
- Gersh BJ, Maron BJ, Bonow RO et al. . 2011 ACCF/AHA Guideline for the Diagnosis and Treatment of Hypertrophic Cardiomyopathy: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Developed in collaboration with the American Association for Thoracic Surgery, American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Failure Society of America, Heart Rhythm Society, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol 2011;58:e212–60. - PubMed
-
- Charron P, Arad M, Arbustini E et al. . Genetic counselling and testing in cardiomyopathies: a position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J 2010;31:2715–26. - PubMed
-
- Maron BJ, Maron MS, Semsarian C. Genetics of hypertrophic cardiomyopathy after 20 years: clinical perspectives. J Am Coll Cardiol 2012;60:705–15. - PubMed
-
- Olivotto I, Girolami F, Ackerman MJ et al. . Myofilament protein gene mutation screening and outcome of patients with hypertrophic cardiomyopathy. Mayo Clin Proc 2008;83:630–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases