

Antibiotics for prelabour rupture of membranes at or near term
- PMID: 25352443
- PMCID: PMC10593255
- DOI: 10.1002/14651858.CD001807.pub2
Antibiotics for prelabour rupture of membranes at or near term
Abstract
Background: Prelabour rupture of the membranes (PROM) at or near term (defined in this review as 36 weeks' gestation or beyond) increases the risk of infection for the woman and her baby. The routine use of antibiotics for women at the time of term PROM may reduce this risk. However, due to increasing problems with bacterial resistance and the risk of maternal anaphylaxis with antibiotic use, it is important to assess the evidence addressing risks and benefits in order to ensure judicious use of antibiotics. This review was undertaken to assess the balance of risks and benefits to the mother and infant of antibiotic prophylaxis for PROM at or near term.
Objectives: To assess the effects of antibiotics administered prophylactically to women with PROM at 36 weeks' gestation or beyond, on maternal, fetal and neonatal outcomes.
Search methods: We searched the Cochrane Pregnancy and Childbirth Group's Trials Register (31 July 2014).
Selection criteria: All randomised trials that compared outcomes for women and infants when antibiotics were administered prophylactically for prelabour rupture of the membranes at or near term, with outcomes for controls (placebo or no antibiotic).
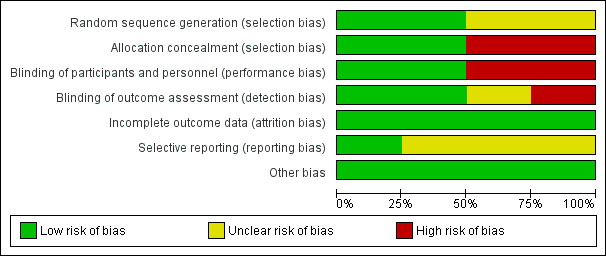
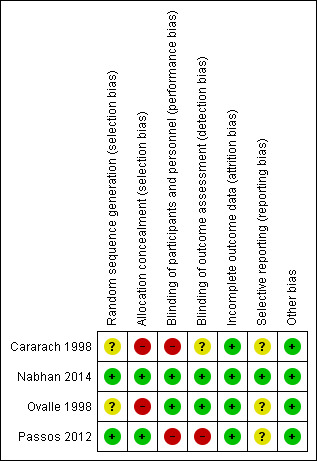
Data collection and analysis: Two review authors independently extracted the data and assessed risk of bias in the included studies. Additional data were received from the investigators of included studies.
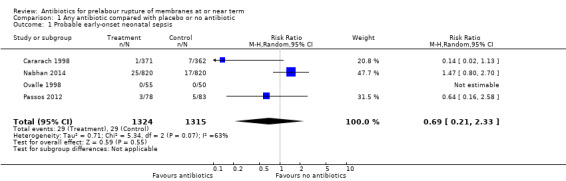
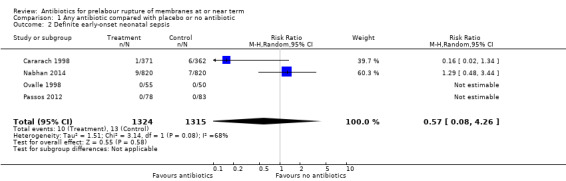
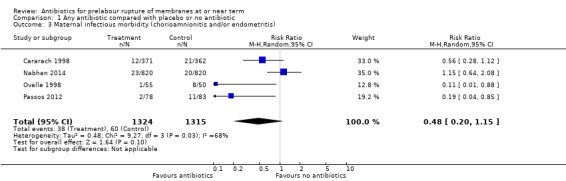
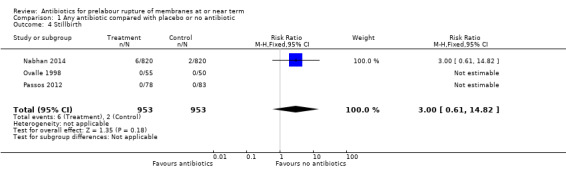
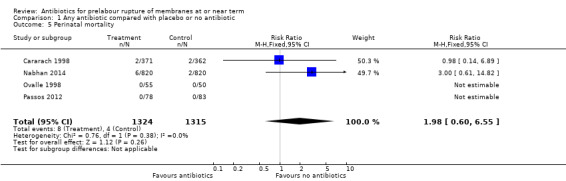
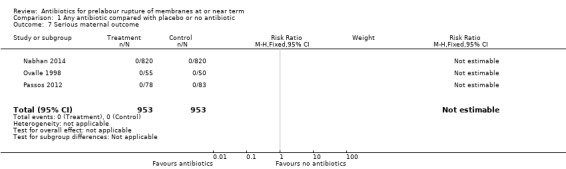
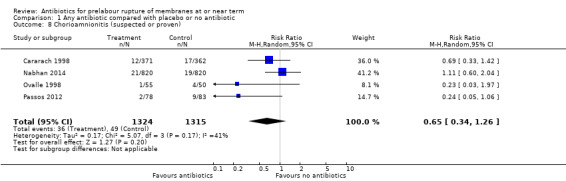
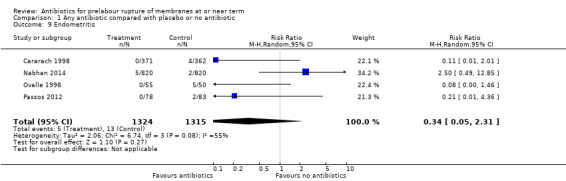
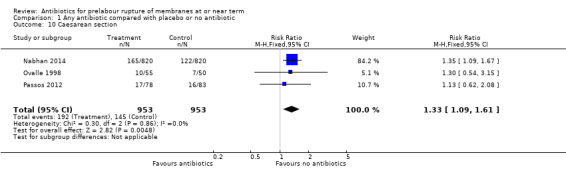
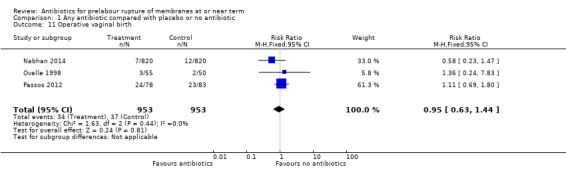
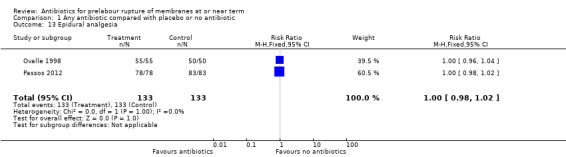
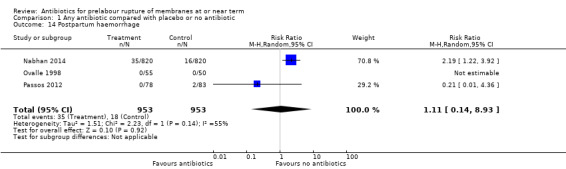
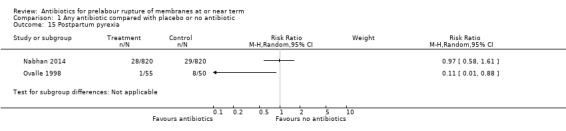
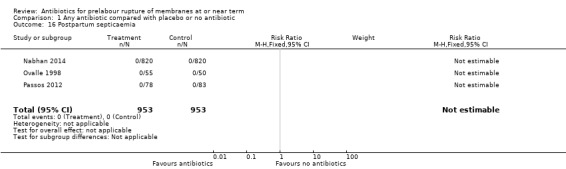
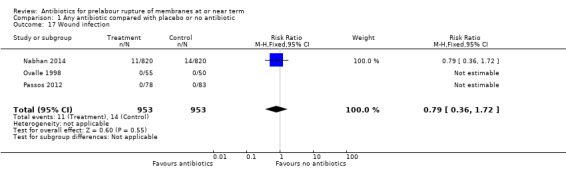
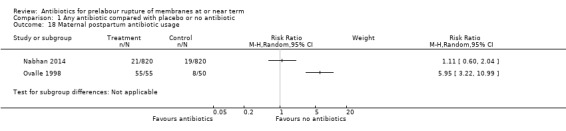
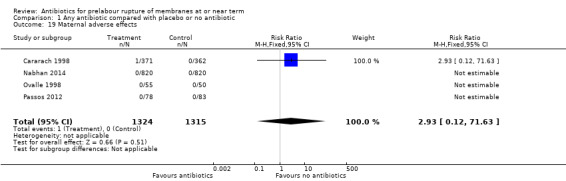
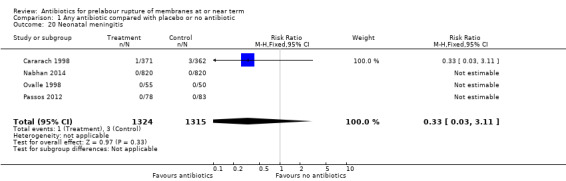
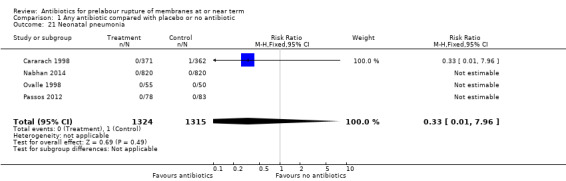
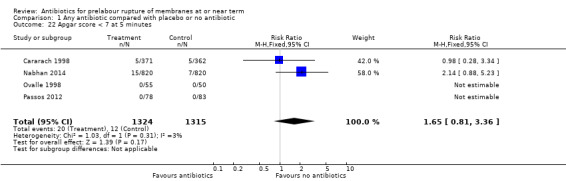
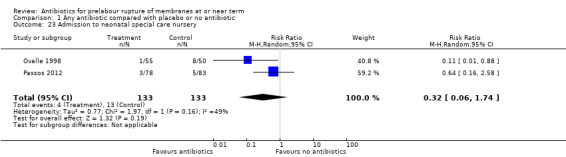
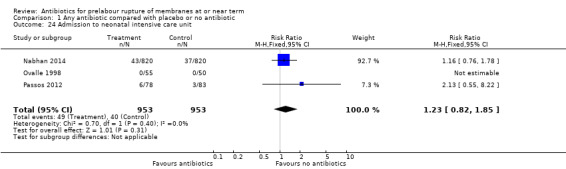
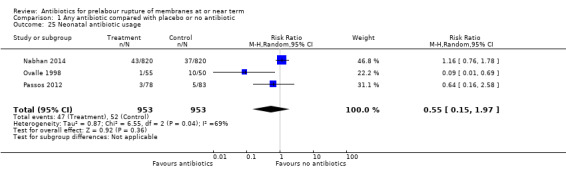
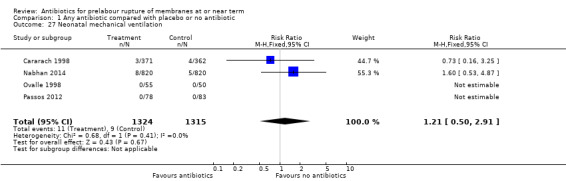
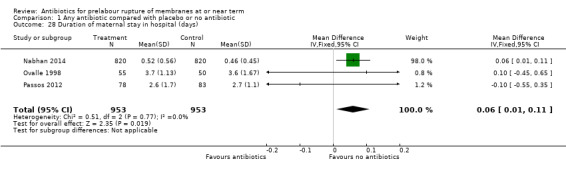
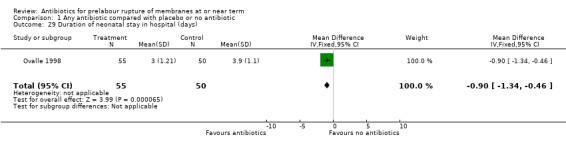
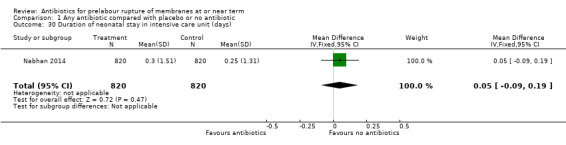
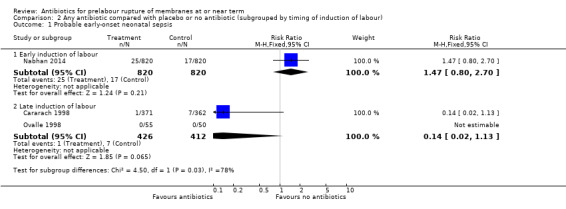
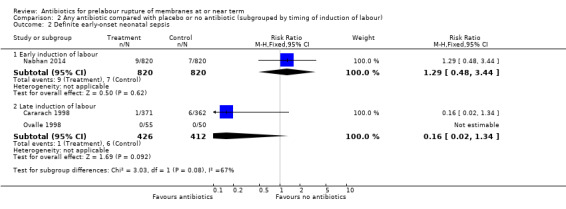
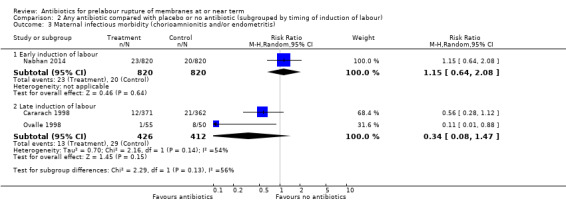
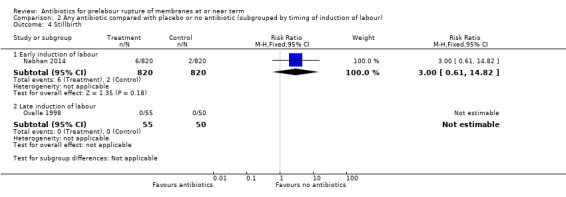
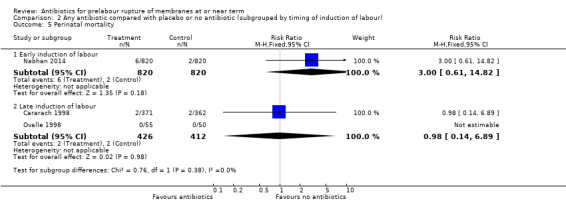
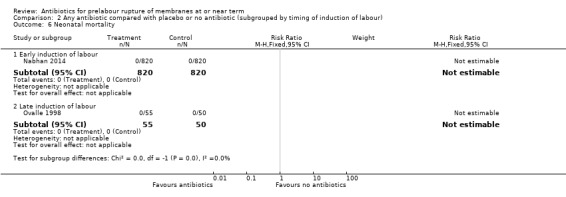
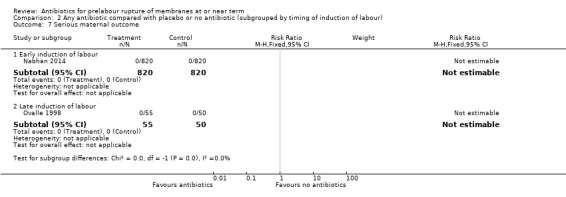
Main results: This update includes an additional two studies involving 1801 women, giving a total of four included studies of 2639 women. Whereas the previous version of this review showed a statistically significant reduction in endometritis with the use of antibiotics, no such effect was shown in this update (average risk ratio (RR) 0.34, 95% confidence interval (CI) 0.05 to 2.31). No differences were shown on the primary outcome measures of probable early-onset neonatal sepsis (average RR 0.69, 95%; CI 0.21 to 2.33); definite early-onset neonatal sepsis (average RR 0.57, 95% CI 0.08 to 4.26); maternal infectious morbidity (chorioamnionitis and/or endometritis) (average RR 0.48, 95% CI 0.20 to 1.15); stillbirth (RR 3.00, 95% CI 0.61 to 14.82); and perinatal mortality (RR 1.98, 95% CI 0.60 to 6.55), though the number of cases in the control group for these outcomes was low. There were no cases of neonatal mortality or serious maternal outcome in the studies assessed. Caesarean section was increased with the use of antibiotics (RR 1.33, 95% CI 1.09 to 1.61) as was duration of maternal stay in hospital (mean difference (MD) 0.06 days, 95% CI 0.01 to 0.11), largely owing to one study of 1640 women where repeat caesarean section, increased baseline hypertension and pre-eclampsia were evident in the antibiotic group, despite random allocation and allocation concealment.Subgroup analyses by timing of induction (early induction versus late induction) showed no difference in either probable or definite early-onset neonatal sepsis in the early induction group (RR 1.47, 95% CI 0.80 to 2.70 and RR 1.29, 95% CI 0.48 to 3.44, respectively) or the late induction group (RR 0.14, 95% CI 0.02 to 1.13 and RR 0.16, 95% CI 0.02 to 1.34, respectively), although there were trends toward reduced probable and definite early-onset neonatal sepsis in the late induction group. A test for subgroup differences confirmed a differential effect of the intervention on probable early-onset neonatal sepsis between the subgroups (Chi² = 4.50, df = 1 (P = 0.03), I² = 77.8%). No difference in maternal infectious morbidity (chorioamnionitis and/or endometritis) was found in either subgroup, though again there was a trend towards reduced maternal infectious morbidly in the late induction group (average RR 0.34, 95% CI 0.08 to 1.47). No differences were shown in stillbirth or perinatal mortality. The quality of the evidence for the primary outcomes using GRADE was judged to be low to very low.
Authors' conclusions: This updated review demonstrates no convincing evidence of benefit for mothers or neonates from the routine use of antibiotics for PROM at or near term. We are unable to adequately assess the risk of short- and long-term harms from the use of antibiotics due to the unavailability of data. Given the unmeasured potential adverse effects of antibiotic use, the potential for the development of resistant organisms, and the low risk of maternal infection in the control group, the routine use of antibiotics for PROM at or near term in the absence of confirmed maternal infection should be avoided.
Conflict of interest statement
None.
Figures
Update of
-
Antibiotics for prelabour rupture of membranes at or near term.Cochrane Database Syst Rev. 2002;(3):CD001807. doi: 10.1002/14651858.CD001807. Cochrane Database Syst Rev. 2002. Update in: Cochrane Database Syst Rev. 2014 Oct 29;(10):CD001807. doi: 10.1002/14651858.CD001807.pub2. PMID: 12137635 Updated.
References
References to studies included in this review
Cararach 1998 {published and unpublished data}
-
- Cararach V, Botet F, Sentis J, Almirall R, Perez‐Picanol E. Administration of antibiotics to patients with rupture of membranes at term: a prospective, randomized, multicentric study. Collaborative Group on PROM. Acta Obstetricia et Gynecologica Scandinavica 1998;77:298‐302. - PubMed
-
- Cararach V, Botet F, Sentis J, Carmona F. A multicenter, prospective and randomized study in premature rupture of membranes (PROM). Maternal and perinatal complications. Proceedings of 13th World Congress of Gynaecology and Obstetrics (FIGO); 1991 Sept 15‐20; Singapore. 1991:267.
-
- Cararach V, Sentis J, Botet F. A multicentre prospective randomized study in premature rupture of the membranes (PROM). Respiratory and infectious complications in the newborn. Proceedings of 12th European Congress of Perinatal Medicine; 1990 September 11‐14; Lyon, France. 1990:216.
Nabhan 2014 {published data only}
-
- Nabhan A. Prophylactic antibiotics for spontaneous prelabor rupture of membranes at term to reduce early neonatal sepsis. http://www.anzctr.org.au/ACTRN12608000501347.aspx [accessed 2 February 2012] 2009.
-
- Nabhan A, Elhilaly A. Antibiotic prophylaxis in prelabor rupture of membranes at term, a randomized trial. Journal of Perinatal Medicine 2013;41(Suppl 1):Abstract no:543.
Ovalle 1998 {published and unpublished data}
-
- Ovalle A, Gomez R, Martinez MA, Giglio MS, Bianchi R, Diaz J, et al. Antibiotic treatment of patients with term premature rupture of membranes reduces the incidence of infection‐related complications. American Journal of Obstetrics and Gynecology 1995;172:301.
-
- Ovalle A, Gomez R, Martinez MA, Giglio MS, Bianchi R, Diaz J, et al. Antibiotic treatment of patients with term premature rupture of membranes: a randomized clinical trial. Prenatal and Neonatal Medicine 1998;3:599‐606.
Passos 2012 {published data only}
-
- Passos F. Antibiotic prophylaxis in prelabor rupture of membranes at term. http://www.clinicaltrials.gov/ct2/show/NCT01633294?term=NCT01633294&... [accessed 28 June 2014] 2012.
-
- Passos F, Cardoso K, Coelho AM, Graca A, Clode N, Mendes LG. Antibiotic prophylaxis in premature rupture of membranes at term: A randomized controlled trial. Obstetrics and Gynecology 2012;120(5):1045‐51. - PubMed
References to studies excluded from this review
Brelje 1966 {published data only}
-
- Brelje MC, Kaltreider DF, Kassir L. The use of vaginal antibiotics in premature rupture of the membranes. American Journal of Obstetrics and Gynecology 1966;94:889‐97. - PubMed
Gordon 1974 {published data only}
-
- Gordon M, Weingold AB. Treatment of patients with premature rupture of the fetal membranes: (a) prior to 32 weeks; (b) after 32 weeks. Premature rupture of the membranes ‐ a rational approach to management. In: Reid DE, Christian CD editor(s). Controversy in Obstetrics and Gynecology II. Philadelphia: WB Saunders Company, 1974:42‐4.
Lebherz 1963 {published data only}
-
- Lebherz TB, Hellman LP, Madding R, Anctil A, Arje SL. Double blind study of premature rupture of the membranes. American Journal of Obstetrics and Gynecology 1963;87:218‐25. - PubMed
Walss Rodriguez 1988 {published data only}
-
- Walss Rodriguez RJ, Navarro Castanon J. Prophylactic antibiotics in premature rupture of the membranes [Antibioticos profilacticos en ruptura prematura de membranas]. Ginecologia y Obstetricia de Mexico 1988;56:339‐42. - PubMed
Additional references
ACOG 2011
-
- American College of Obstetricians and Gynecologists. ACOG Practice Bulletin No. 120: Use of prophylactic antibiotics in labor and delivery. Obstetrics and Gynecology 2011;117(6):1472‐83. - PubMed
Cammu 1990
-
- Cammu H, Verlaenen H, Derde M. Premature rupture of membranes at term in multiparous women: a hazard?. Obstetrics & Gynecology 1990;76:671‐4. - PubMed
Dare 2006
Duff 1998
-
- Duff P. Premature rupture of the membranes in term patients: induction of labor versus expectant management. Clinical Obstetrics and Gynecology 1998;41(4):883‐91. - PubMed
Edwards 2001
-
- Edwards R, Clark P, Duff P. Intrapartum antibiotic prophylaxis with either penicillin or ampicillin may increase the rate of neonatal sepsis caused by ampicillin‐resistant Gram‐negative bacteria. American Journal of Obstetrics and Gynecology 2001;185:S190.
Ezra 2004
-
- Ezra Y, Michaelson‐Cohen R, Abramov Y, Rojansky N. Prelabor rupture of the membranes at term: when to induce labor?. European Journal of Obstetrics & Gynecology and Reproductive Biology 2004;115:23‐7. - PubMed
Gates 2004
-
- Gates S, Brocklehurst P. How should randomised trials including multiple pregnancies be analysed?. BJOG: an international journal of obstetrics and gynecology 2004;111(3):213‐29. - PubMed
GRADE 2008 [Computer program]
-
- Brozek J, Oxman A, Schünemann H. GRADEpro. Version 3.6. The Cochrane Collaboration, 2008.
Hannah 1996
-
- Hannah ME, Ohlsson A, Farine D, Hewson SA, Hodnett ED, Myhr TL, et al. Induction of labor compared with expectant management for prelabour rupture of the membranes at term. New England Journal of Medicine 1996;334:1005‐10. - PubMed
Heim 1991
-
- Heim K, Alge A, Marth C. Anaphylactic reaction to ampicillin and severe complications in the fetus. Lancet 1991;337:859‐60. - PubMed
Higgins 2011
-
- Higgins JPT, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Ingemarsson 1996
-
- Ingemarsson I. Controversies: premature rupture of membranes at term‐‐no advantage of delaying induction >24 hours. Journal of Perinatal Medicine 1996;24(6):573‐9. - PubMed
Jao 2006
-
- Jao MS, Cheng PJ, Shaw SW, Soong YK. Anaphylaxis to cefazolin during labor secondary to prophylaxis for group B Streptococcus: a case report. Journal of Reproductive Medicine 2006;51(8):655‐8. - PubMed
Lin 1999
-
- Lin FY, Weisman LE, Azimi PH, Regan JA, Philips JB, Clark P, et al. Antibiotic susceptibility of invasive group B streptococci from neonates with early‐onset disease ‐ a multi center study 1995‐97. Proceedings of Pediatric Academic Societies' Annual Meeting; 1999 May 1‐May 4, San Francisco, CA. 1999.
Marowitz 2007
-
- Marowitz A, Jordan R. Midwifery management of prelabor rupture of membranes at term. Journal of Midwifery and Women’s Health 2007;52(3):199–206. - PubMed
Marshall 2002
-
- Marshall JF, Vasilenko P. Classification of prematurity by gestational age: a concept now mature. Obstetrics & Gynecology 2002;99(4 Suppl):855.
Moore 2006
-
- Moore RM, Mansour JM, Redline RW, Mercer BM, Moore JJ. The physiology of fetal membrane rupture: insight gained from the determination of physical properties. Placenta 2006;27(11‐12):1037‐51. - PubMed
Mozurkewich 2006
-
- Mozurkewich E. Prelabor rupture of membranes at term: induction techniques. Clinical Obstetrics and Gynecology 2006;49(3):672‐83. - PubMed
Neerhoff 1999
-
- Neerhoff GM, Cravello C, Haney EI, Silver RK. Timing of labor induction after premature rupture of membranes between 32 and 36 weeks' gestation. American Journal of Obstetrics and Gynecology 1999;180(2):349‐52. - PubMed
Newton 1993
-
- Newton ER. Chorioamnionitis and intraamniotic infection. Clinical Obstetrics and Gynecology 1993;366:795‐808. - PubMed
Ohlsson 2014
Reti 2007
-
- Reti NG, Lappas M, Riley C, Wlodek ME, Permezel M, Walker S, et al. Why do membranes rupture at term? Evidence of increased cellular apoptosis in the supracervical fetal membranes. American Journal of Obstetrics and Gynecology 2007;196(5):484.e1‐484.e10. - PubMed
RevMan 2014 [Computer program]
-
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Romero 1992
-
- Romero R, Mazor M, Morrotti R, Avila C, Oyarzun E, Insunza A, et al. Microbial invasion of the amniotic cavity in spontaneous rupture of membranes at term. American Journal of Obstetrics and Gynecology 1992;166(1):129‐33. - PubMed
Schunemann 2009
-
- Schunemann HJ. GRADE: from grading the evidence to developing recommendations. A description of the system and a proposal regarding the transferability of the results of clinical research to clinical practice [GRADE: Von der Evidenz zur Empfehlung. Beschreibung des Systems und Losungsbeitrag zur Ubertragbarkeit von Studienergebnissen]. Zeitschrift fur Evidenz, Fortbildung und Qualitat im Gesundheitswesen 2009;103(6):391‐400. - PubMed
Stoll 2002
-
- Stoll BJ, Hansen N, Fanaroff AA, Wright LL, Carlo WA, Ehrenkranz RA, et al. Changes in pathogens causing early‐onset sepsis in very‐low‐birth‐weight Infants. New England Journal of Medicine 2002;347:240–7. - PubMed
Tran 2007
-
- Tran SH, Cheng YW, Kaimal AJ, Caughey AB. Length of rupture of membranes in the setting of premature rupture of membranes at term and infectious maternal morbidity. American Journal of Obstetrics and Gynecology 2008;198(6):700.e1–700.e5. - PubMed
Yelland 2011
-
- Yelland LN, Saltera AB, Ryana P, Makridesb M. Analysis of binary outcomes from randomised trials including multiple births: when should clustering be taken into account?. Paediatric and Perinatal Epidemiology 2011;25:283–97. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous